

If you desire to fill out fidelity durable power of attorney affidavit and indemnification form, you won't need to install any kind of software - simply try using our PDF editor. We are focused on providing you the absolute best experience with our tool by continuously releasing new capabilities and enhancements. Our tool is now much more useful with the newest updates! At this point, working with PDF files is easier and faster than ever. To get started on your journey, take these simple steps:
Step 1: Firstly, open the pdf tool by clicking the "Get Form Button" in the top section of this site.
Step 2: This tool offers you the opportunity to customize nearly all PDF documents in various ways. Change it by adding personalized text, correct what's already in the file, and add a signature - all readily available!
This form will require particular details to be typed in, thus you must take the time to type in exactly what is required:
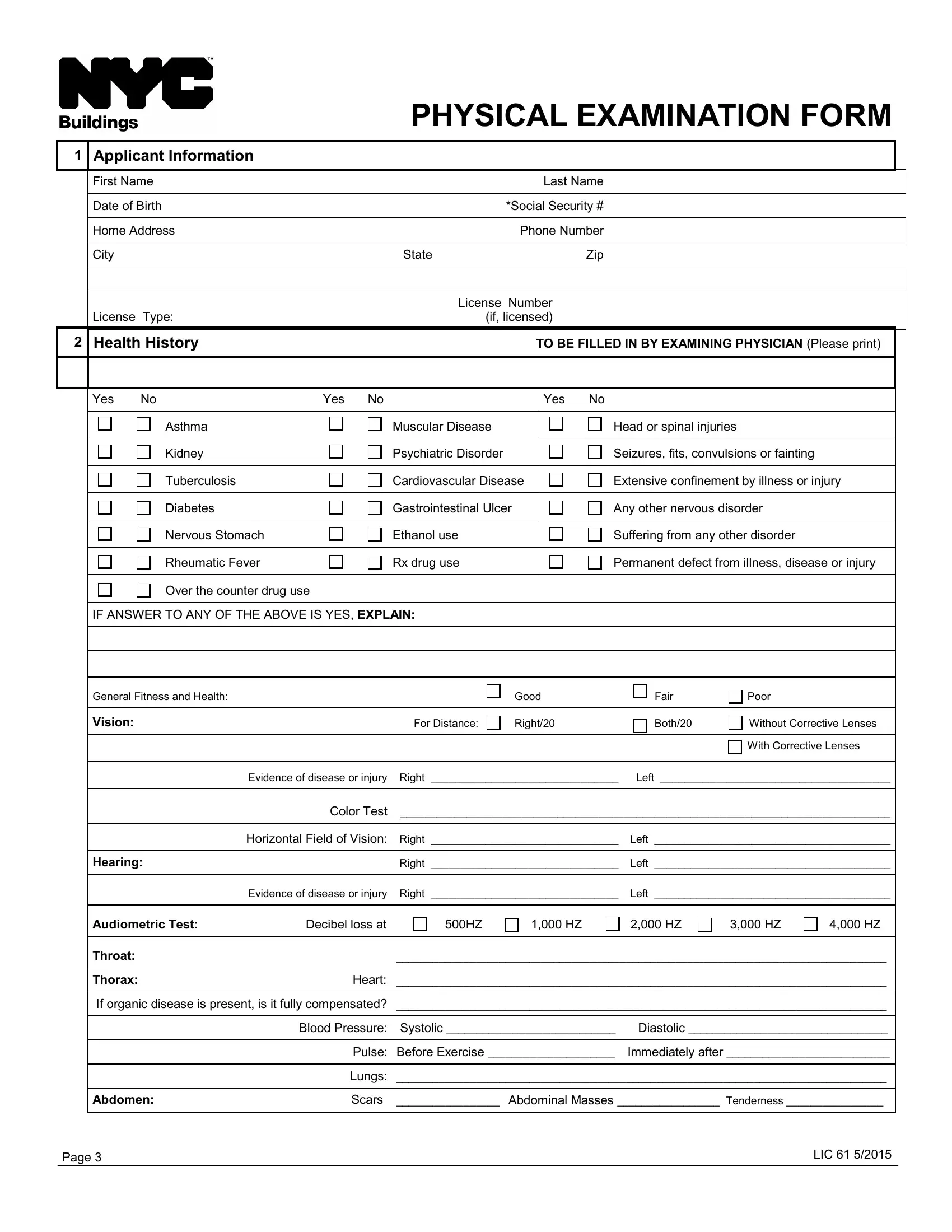
1. To start off, while filling out the fidelity durable power of attorney affidavit and indemnification form, start with the area that features the next fields:
2. Soon after the prior section is completed, go on to enter the suitable information in all these: IF ANSWER TO ANY OF THE ABOVE IS, General Fitness and Health, Vision, Good, Fair, Poor, For Distance Right, Both, Without Corrective Lenses, With Corrective Lenses, Evidence of disease or injury, Left, Hearing, Right Left, and Horizontal Field of Vision Right.
3. This subsequent section should also be relatively uncomplicated, Throat Thorax Heart If organic, Page, and LIC - these blanks is required to be completed here.
4. Completing PHYSICAL EXAMINATION FORM CONTD, Hernia Yes No, If so where, Is truss worn, Gastrointestinal Ulceration or, GenitoUrinary Scars, Urinal Discharge, Reflexes Rhomberg, Knee Jerks, Pupillary, Light R, Accommodation, Right Normal, Increased, and Absent is paramount in the fourth form section - ensure to take your time and take a close look at each blank area!
5. This last section to conclude this PDF form is pivotal. Ensure to fill out the mandatory form fields, for instance Physician TO BE FILLED IN BY, Name of Physician, Address of Physician City, Phone of Physician, State, Zip, Physicians Signature, Date, Physicians Clearance, Physicians Clearance TO BE FILLED, I certify that I have examined, with the knowledge of hisher, Qualified to perform work in their, Qualified only when wearing a, and A complete examination form for, prior to using the form. Failing to do this could generate an incomplete and possibly incorrect document!
Be extremely attentive while completing Date and Physicians Clearance, since this is where many people make errors.
Step 3: Before moving on, check that form fields were filled in the correct way. When you are satisfied with it, click on “Done." Join us now and easily get fidelity durable power of attorney affidavit and indemnification form, available for downloading. Every single modification made is conveniently saved , which enables you to change the form later if required. We don't sell or share the details that you use whenever dealing with documents at FormsPal.