

physical form 2019 print can be filled in online without any problem. Simply make use of FormsPal PDF editor to complete the task quickly. Our expert team is constantly endeavoring to expand the tool and enable it to be much easier for users with its multiple features. Benefit from the current revolutionary possibilities, and find a heap of emerging experiences! If you are seeking to begin, here is what it takes:
Step 1: Hit the "Get Form" button above on this page to access our tool.
Step 2: With the help of our state-of-the-art PDF tool, you can actually accomplish more than merely complete blanks. Try each of the features and make your docs appear sublime with custom text put in, or adjust the file's original content to perfection - all that supported by the capability to add stunning images and sign the file off.
For you to complete this document, ensure you provide the required information in each and every blank field:
1. While completing the physical form 2019 print, be sure to complete all of the essential blanks in its corresponding form section. This will help to facilitate the process, which allows your information to be processed promptly and accurately.
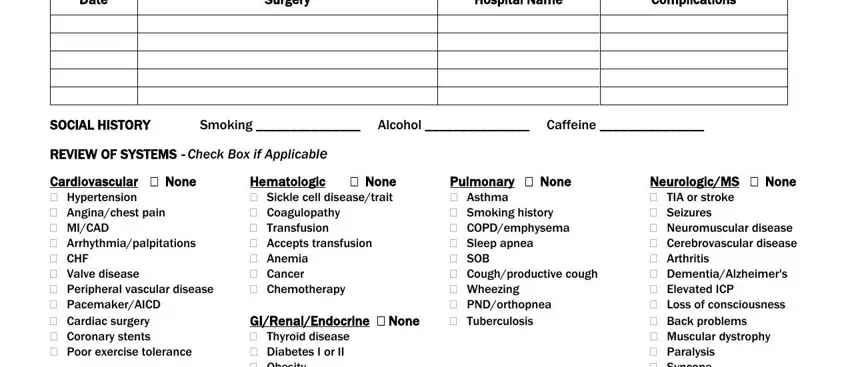
2. Right after the last array of fields is done, go to type in the relevant details in these: Date, Surgery, Hospital Name, Complications, Smoking Alcohol Caffeine, SOCIAL HISTORY REVIEW OF SYSTEMS, None Hematologic Sickle cell, Pulmonary None Asthma Smoking, and NeurologicMS None TIA or stroke.
Regarding Hospital Name and Smoking Alcohol Caffeine, make sure you get them right in this section. The two of these are the most significant fields in the PDF.
3. The next stage is normally hassle-free - fill out all the form fields in SOCIAL HISTORY REVIEW OF SYSTEMS, None Hematologic Sickle cell, Tubal ligation, Pulmonary None Asthma Smoking, NeurologicMS None TIA or stroke, and Page of to conclude this segment.
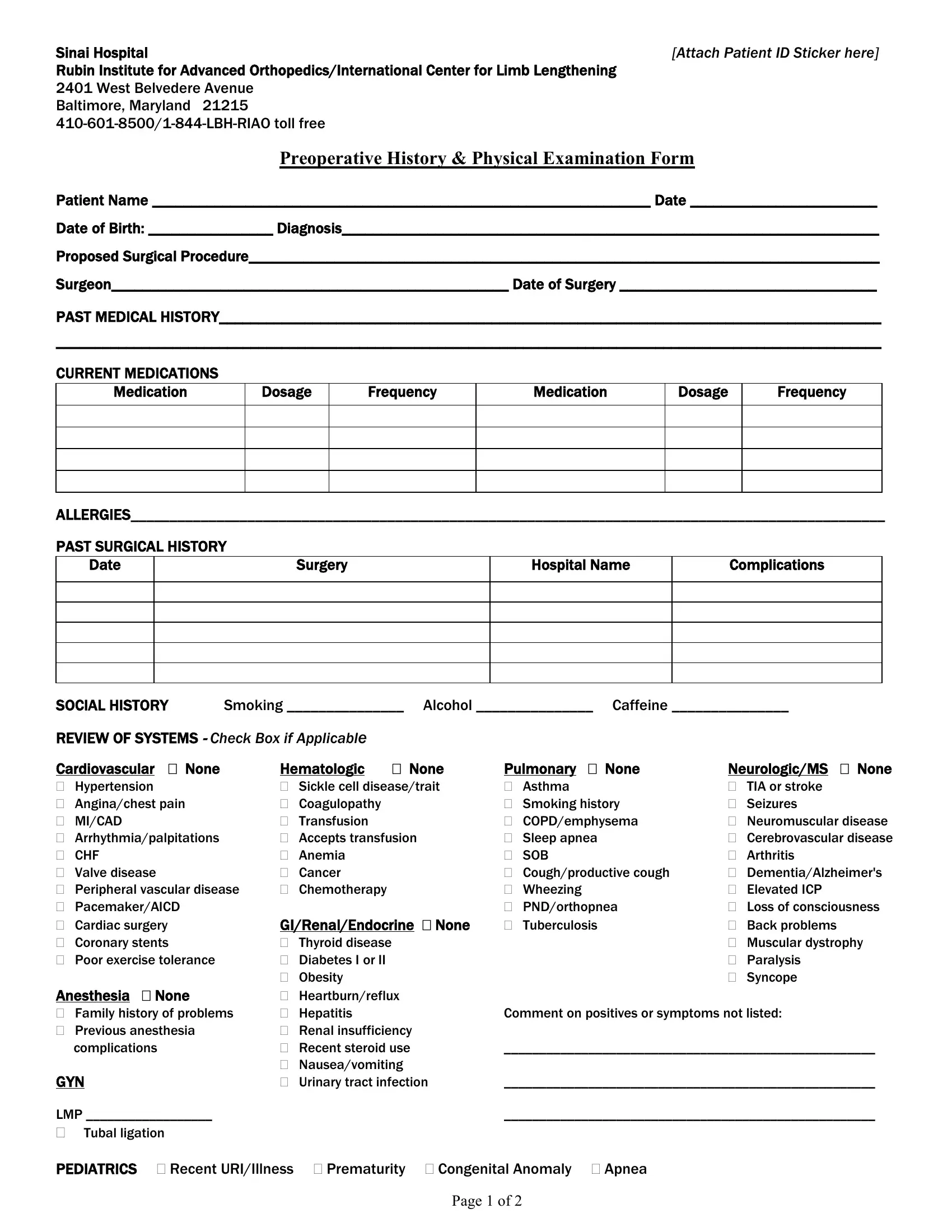
4. To move forward, this section requires completing a couple of empty form fields. Examples of these are Sinai Hospital Rubin Institute for, Patient Name Date of Birth, Attach Patient ID Sticker here, Preoperative History Physical, PHYSICAL EXAM, Sex, Race, Age, Height, Weight KG, Pulse, Resp, Temp, EOMI, and No JVD, which you'll find integral to going forward with this particular document.
5. To finish your document, the particular segment requires several additional blank fields. Entering No Clubbing, Lungs CTA BL, No Hepatosplenomegaly, Abd Benign Normoactive BS, General appearance HEENT Abnormal, Deferred, NML Muscle Tone, Heme negative, CN IIXII intact, NML Strength, No Cyanosis, No masses, NML Mood, and No Edema will conclude everything and you'll be done in an instant!
Step 3: Confirm that the details are correct and click "Done" to conclude the task. Try a free trial plan at FormsPal and acquire instant access to physical form 2019 print - downloadable, emailable, and editable in your FormsPal cabinet. We don't sell or share the information that you enter whenever dealing with forms at FormsPal.