Our finest software engineers have worked together to develop the PDF editor that one could go with. This specific software makes it simple to obtain polst form documents shortly and without problems. This is certainly everything you should undertake.
Step 1: Press the "Get Form Now" button to begin the process.
Step 2: You can find all the options that you can take on the document when you have entered the polst form editing page.
These particular areas are what you will have to create to get the finished PDF form.
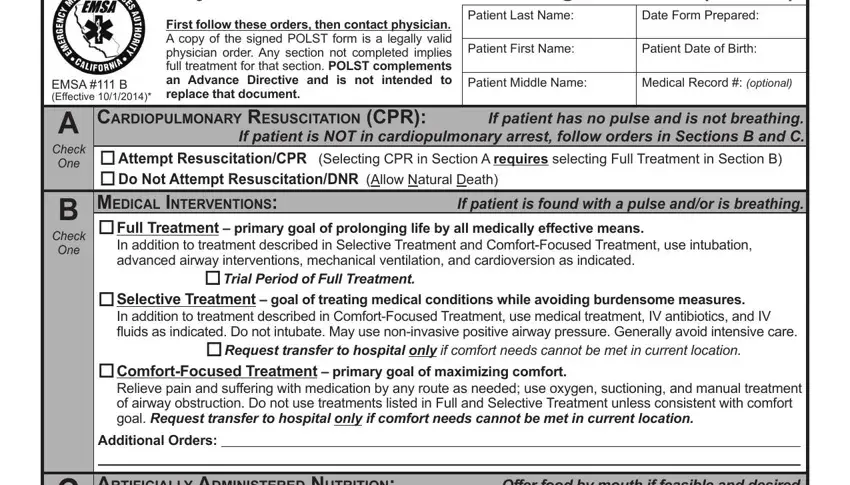
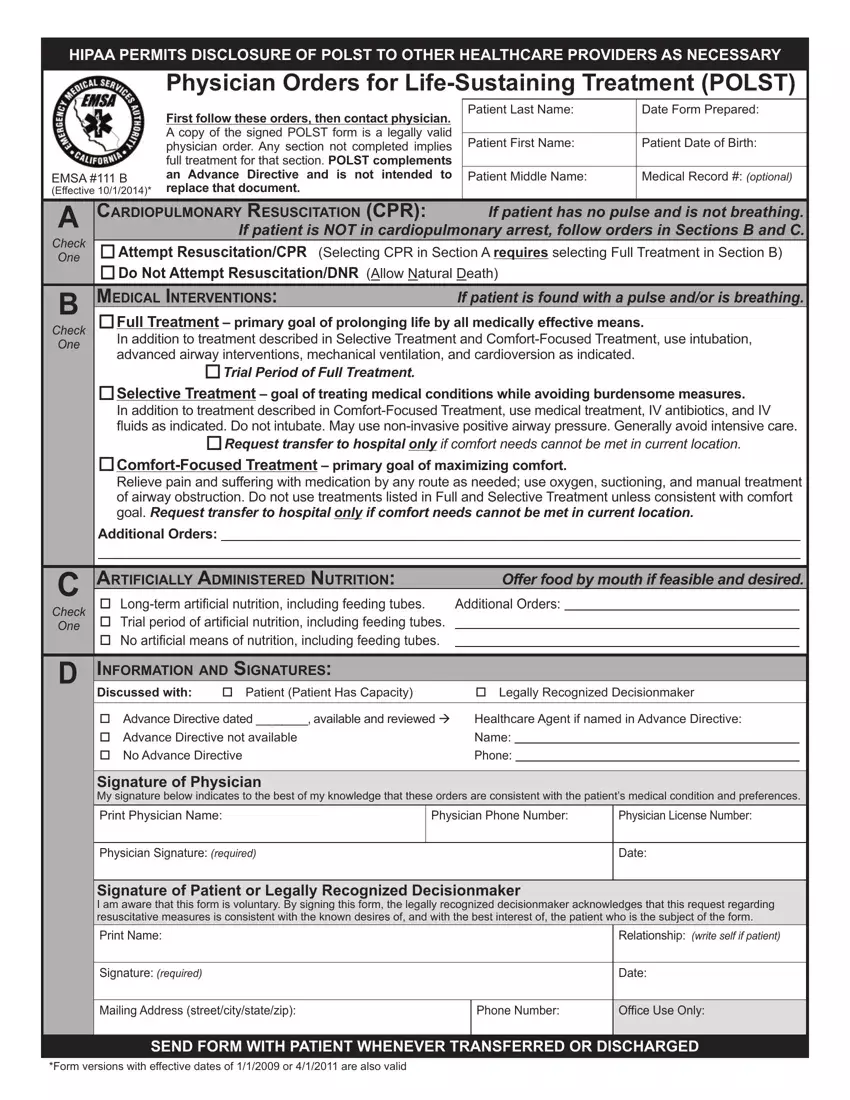
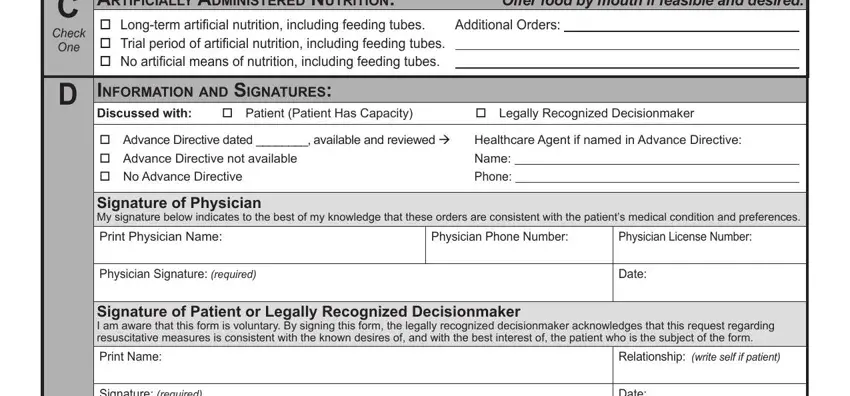
You have to type in the necessary information in the Check One, artIfICIally admInIStered, Additional Orders, Offer food by mouth if feasible, D InformatIon and SIgnatureS, Discussed with o Patient Patient, o Advance Directive dated, Healthcare Agent if named in, Signature of Physician My, Print Physician Name, Physician Phone Number, Physician License Number, Physician Signature required, Date, and Signature of Patient or Legally field.
You can be requested to provide the details to help the platform fill in the box Signature required, Date, Mailing Address streetcitystatezip, Phone Number, Ofice Use Only, SEND FORM WITH PATIENT WHENEVER, and Form versions with effective dates.

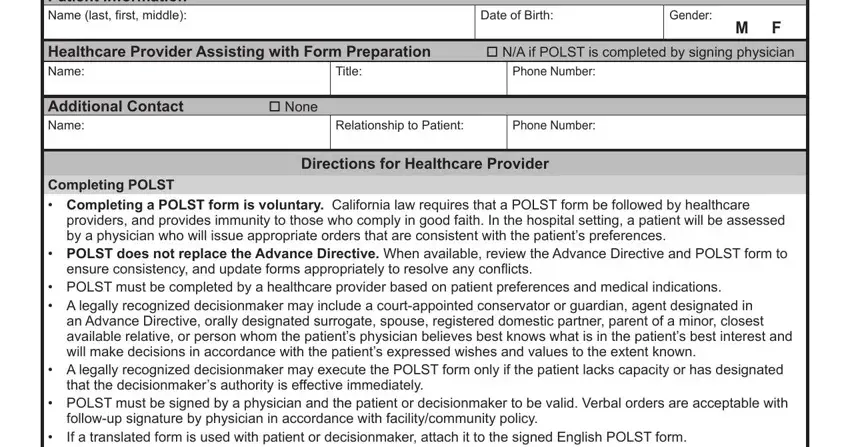
Make sure you specify the rights and obligations of the parties in the Patient Information Name last irst, Date of Birth, Gender M F, Healthcare Provider Assisting with, Phone Number, Title, Additional Contact o None Name, Relationship to Patient, Phone Number, Directions for Healthcare Provider, Completing POLST Completing a, providers and provides immunity to, POLST does not replace the, ensure consistency and update, and POLST must be completed by a part.
Step 3: Hit the "Done" button. Now you may upload your PDF file to your electronic device. Aside from that, you'll be able to forward it through email.
Step 4: Attempt to generate as many copies of your form as you can to stay away from potential problems.
