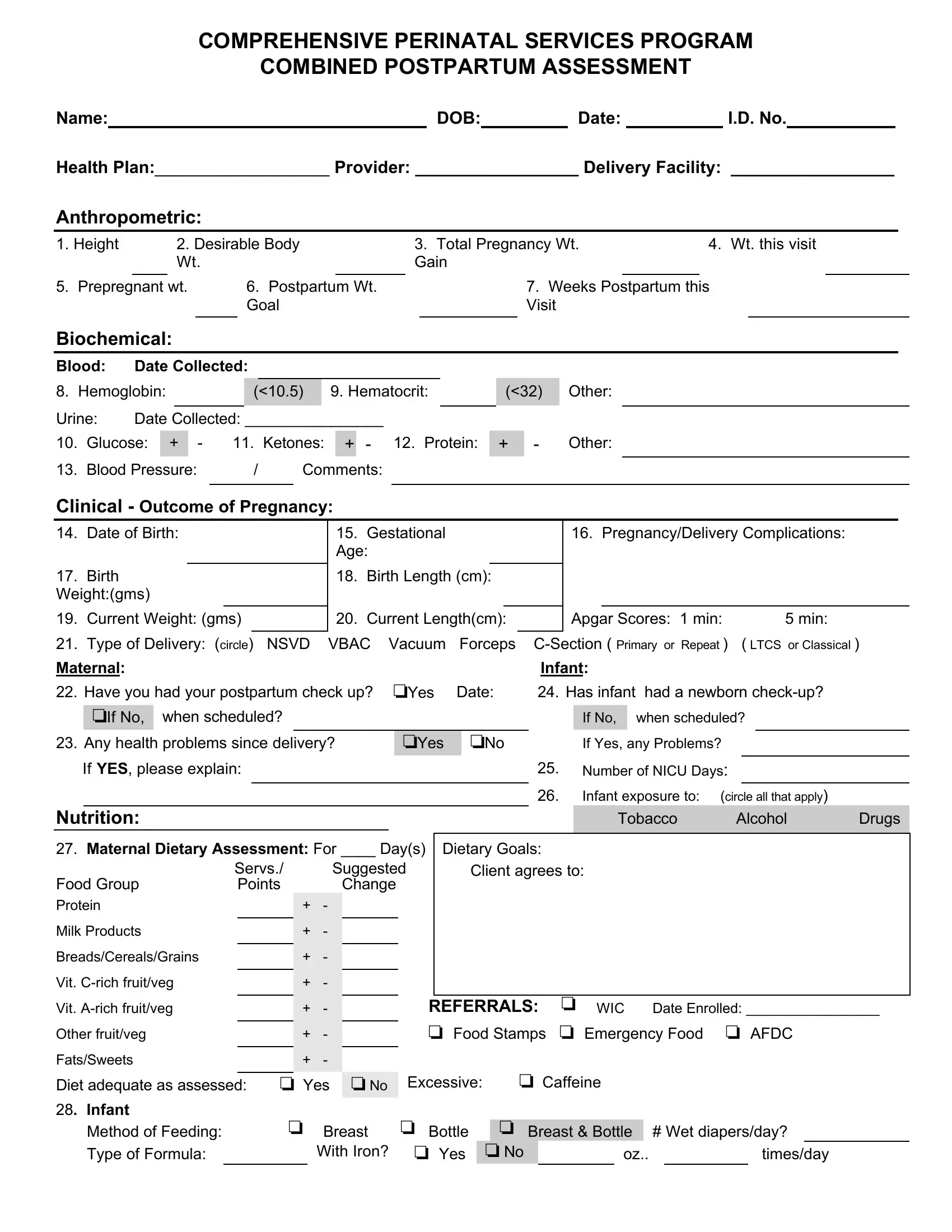
The Postpartum Assessment Example Form is a vital tool within the Comprehensive Perinatal Services Program, designed to guide healthcare providers in conducting thorough postpartum evaluations. This detailed form encompasses various elements crucial for assessing the well-being of both the mother and the newborn, subsequent to delivery. Key areas of assessment include anthropometric measurements, such as height, body weight goals, and postpartum weight, which offer insights into the physical recovery of the mother. Biochemical data, including hemoglobin and glucose levels, provide information on the mother's post-delivery health status. Furthermore, the form captures significant pregnancy and delivery details, including the outcome of the pregnancy, any complications, and the type of delivery, alongside the newborn's health metrics such as birth weight and current measurements. The form delves into maternal and infant nutrition, addressing dietary assessments and feeding methods, which are crucial for both mother and child's well-being. It also explores psychosocial aspects, inquiring about the mother’s emotional state, adjustments within the household, and the support system available for the new family. Additionally, healthcare referrals, educational needs, and a plan encompassing client goals and interventions are outlined. This comprehensive approach ensures that both the mother and the infant receive the care and support necessary during the critical postpartum period.
| Question | Answer |
|---|---|
| Form Name | Postpartum Assessment Example Form |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | postnatal assessment formates, postnatal assessment format, postnatal assessment format pdf, postpartum charting template |
