We've applied the efforts of the best programmers to create the PDF editor you may want to take advantage of. The app will permit you to fill out the ems patient care report pdf file effortlessly and don’t waste valuable time. All you should undertake is follow these straightforward instructions.
Step 1: Select the button "Get Form Here".
Step 2: Once you've entered the ems patient care report pdf editing page you'll be able to notice all the options you may conduct with regards to your template within the upper menu.
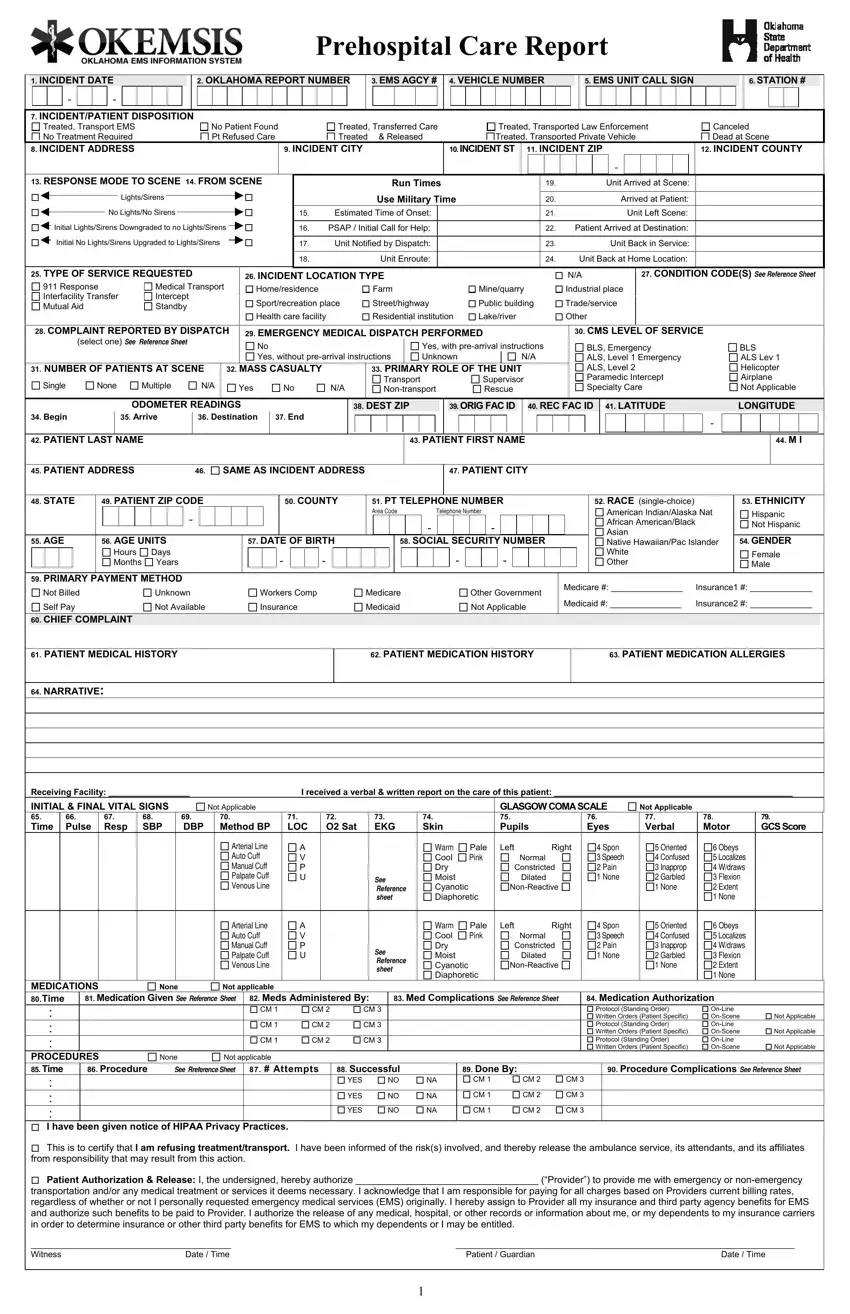
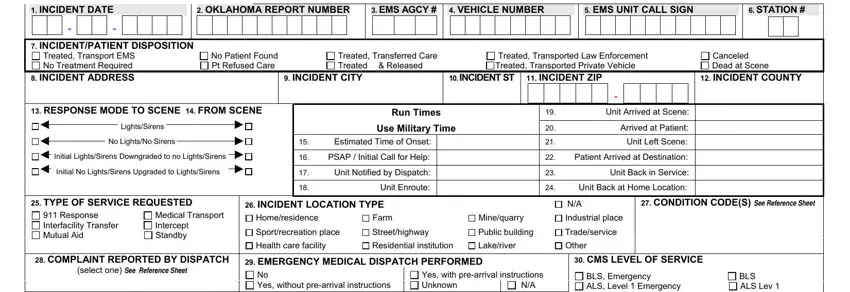
These particular parts are in the PDF file you'll be completing.
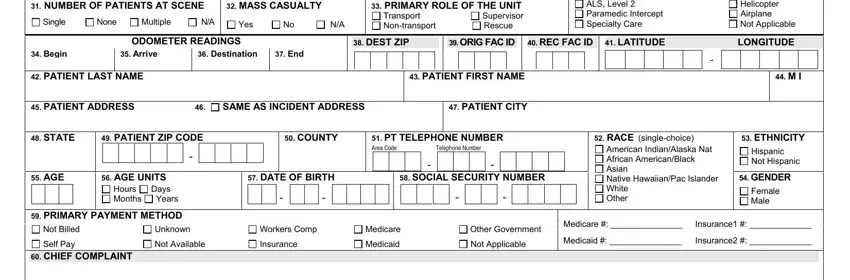
In the NUMBER, OF, PATIENTS, AT, SCENE Single, None, Multiple, MASS, CASUALTY Yes, PRIMARY, ROLE, OF, THE, UNIT Transport, Non, transport Supervisor, Rescue ODOMETER, READINGS DE, ST, ZIP ORIG, F, ACID RE, CF, ACID Begin, PATIENT, LASTNAME and Arrive box, note down your data.
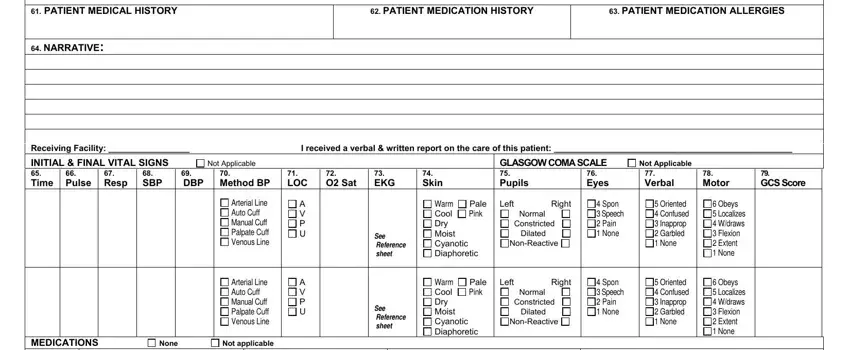
Make sure you emphasize the vital data from the PATIENT, MEDICATION, HISTORY PATIENT, MEDICATION, ALLERGIES Receiving, Facility Not, Applicable, GLASGOW, COMA, SCALE INITIAL, FINAL, VITAL, SIGNS, TimeD, BP Pulse, Resp, SBP, Method, BP LOC, OS, at None, Not, applicable A, VP, U and A, VP, U area.
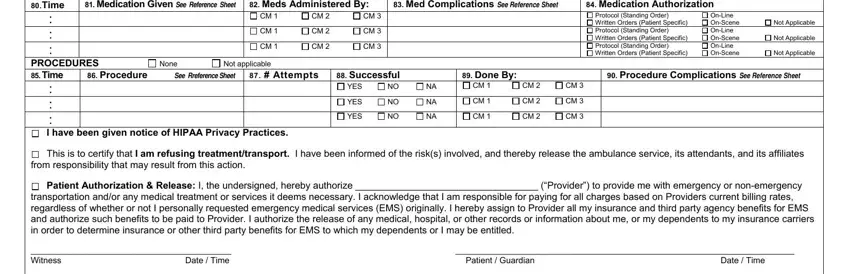
Within the part Medication, Given, See, Reference, Sheet Medication, Authorization Meds, Administered, By Med, Complications, See, Reference, Sheet Attempts, Successful, Done, By YES, YES, YES, Not, Applicable Not, Applicable Not, Applicable MEDICATIONS, Time, PROCEDURES, Time and None, place the rights and responsibilities of the sides.
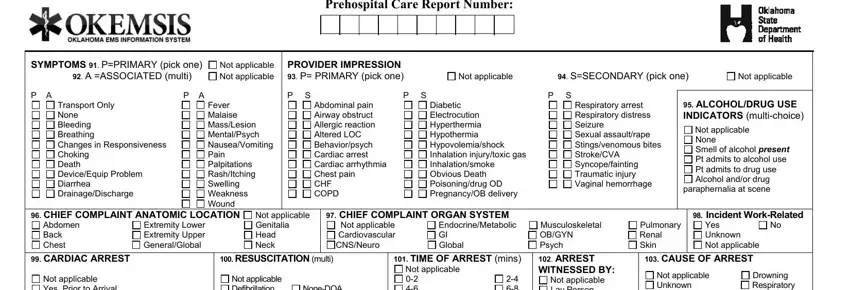
Finish the form by looking at the next sections: Pre, hospital, Care, Report, Number Not, applicable, Not, applicable PROVIDER, IMPRESSION, P, PRIMARY, pick, one Not, applicable S, SECONDARY, pick, one Not, applicable ALCOHOL, DRUG, USE, INDICATORS, multi, choice paraphernalia, at, scene CHIEF, COMPLAINT, ANATOMIC, LOCATION Abdomen, Back, Chest Not, applicable, Genitalia, Head, Neck CHIEF, COMPLAINT, ORGAN, SYSTEM Incident, Work, Related Not, applicable, Cardiovascular, CNS, Neuro and Endocrine, Metabolic, GI, Global
Step 3: Choose the "Done" button. Then, you can transfer your PDF file - save it to your device or forward it by means of electronic mail.
Step 4: Ensure that you stay away from future problems by getting as much as a couple of copies of the form.
