
You'll be able to fill out 2009 without difficulty using our online PDF editor. The editor is constantly updated by our staff, getting new functions and growing to be better. To get the ball rolling, go through these basic steps:
Step 1: Press the "Get Form" button above. It's going to open up our tool so that you could start completing your form.
Step 2: The editor helps you customize PDF files in various ways. Transform it by writing customized text, correct what's already in the document, and include a signature - all readily available!
Filling out this PDF generally requires attentiveness. Make certain every blank is completed accurately.
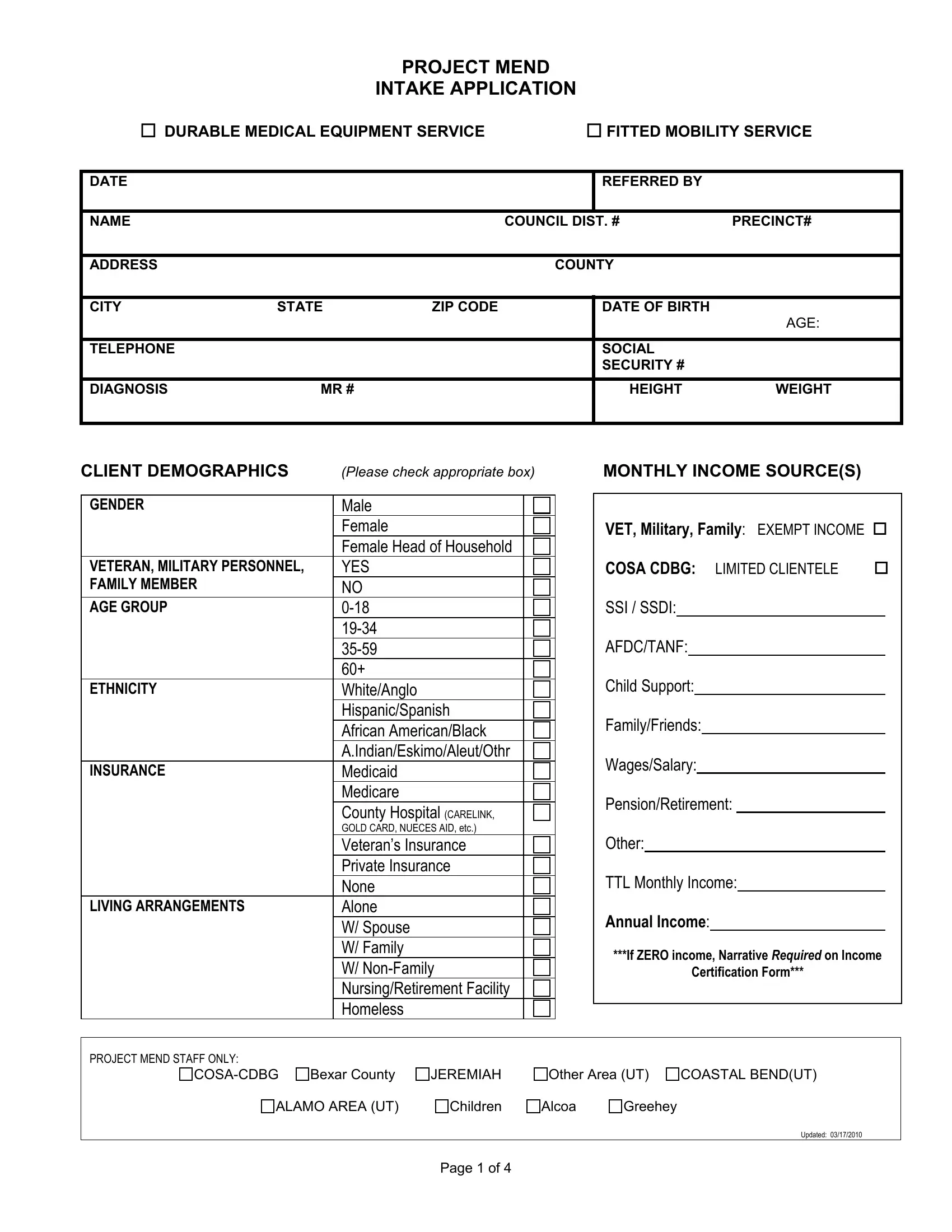
1. The 2009 usually requires particular information to be entered. Be sure the subsequent fields are filled out:
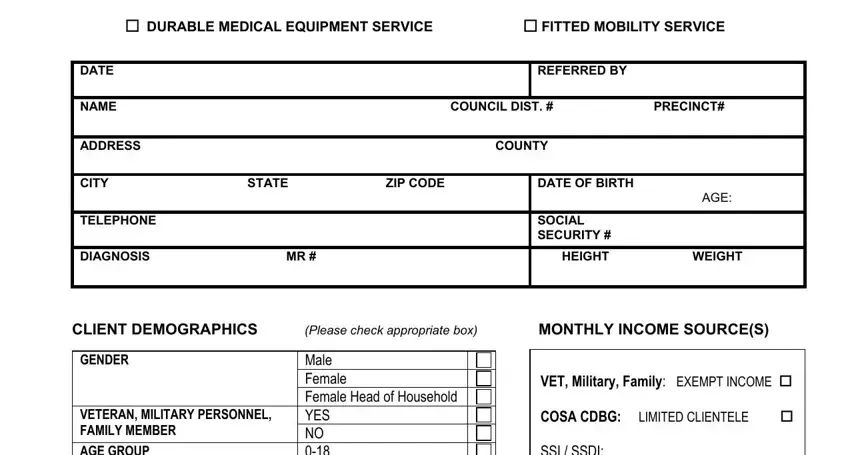
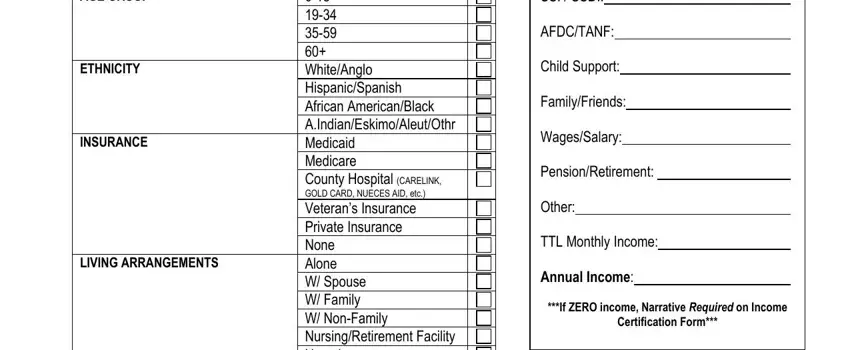
2. After this section is completed, go on to enter the suitable details in these - AGE GROUP, ETHNICITY, INSURANCE, LIVING ARRANGEMENTS, Male Female Female Head of, VET Military Family EXEMPT INCOME, If ZERO income Narrative Required, and Certification Form.
3. Completing PROJECT MEND STAFF ONLY, COSACDBG Bexar County, JEREMIAH Other Area UT COASTAL, ALAMO AREA UT Children Alcoa, Updated, and Page of is essential for the next step, make sure to fill them out in their entirety. Don't miss any details!

As to COSACDBG Bexar County and JEREMIAH Other Area UT COASTAL, ensure you get them right in this section. These are surely the most important fields in the page.
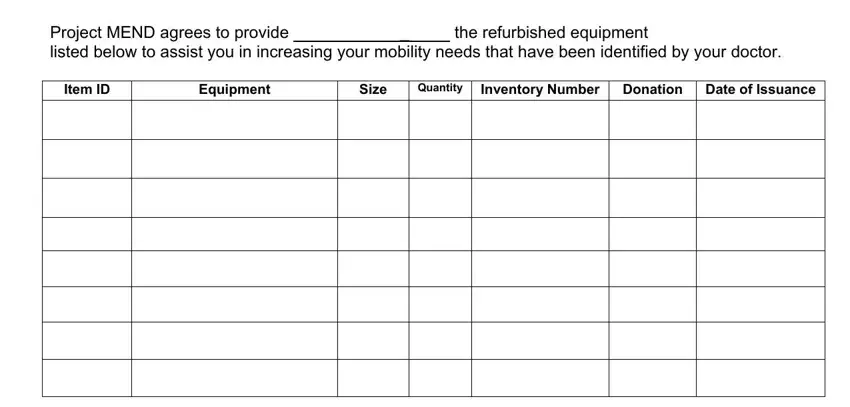
4. This next section requires some additional information. Ensure you complete all the necessary fields - Project MEND agrees to provide, the refurbished equipment, Item ID, Equipment, Size, Quantity, Inventory Number Donation Date of, and Conditions of the Service - to proceed further in your process!
5. Since you get close to the end of your file, there are a couple extra requirements that need to be fulfilled. Specifically, address and phone number should, Conditions of the Service, use this equipment which has been, I acknowledge that I have received, examined the equipment to inspect, of this equipment, ClientRepresentative Project MEND, Date, Date, and PROJECT MEND Staff ONLY Original must be filled out.
Step 3: After double-checking your entries, hit "Done" and you're good to go! Go for a 7-day free trial option at FormsPal and get immediate access to 2009 - download, email, or edit inside your personal account. With FormsPal, you can fill out documents without the need to get worried about database breaches or records being distributed. Our secure platform ensures that your private information is stored safe.