
Dealing with PDF files online can be easy using our PDF editor. You can fill out Csd 43 Form here with no trouble. FormsPal expert team is relentlessly working to expand the editor and make it even easier for people with its cutting-edge functions. Take your experience one stage further with continuously improving and interesting options available today! With just several simple steps, it is possible to begin your PDF journey:
Step 1: Firstly, open the tool by clicking the "Get Form Button" above on this site.
Step 2: As you open the PDF editor, you will find the document ready to be filled in. Apart from filling in different fields, you could also perform various other actions with the PDF, specifically writing your own textual content, editing the initial textual content, adding images, placing your signature to the PDF, and a lot more.
As a way to finalize this PDF form, make sure you provide the necessary information in each area:
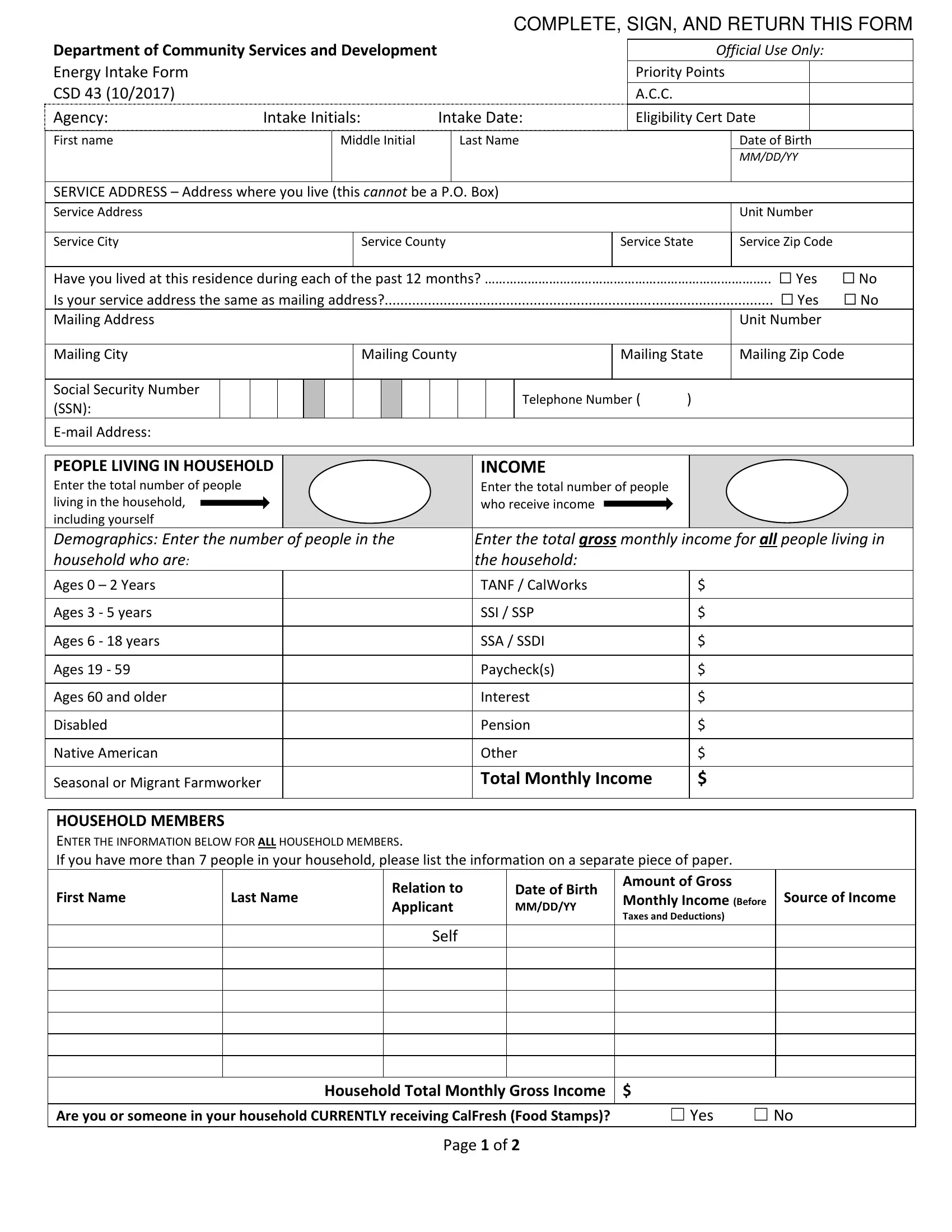
1. To get started, once filling out the Csd 43 Form, start out with the page containing next blank fields:
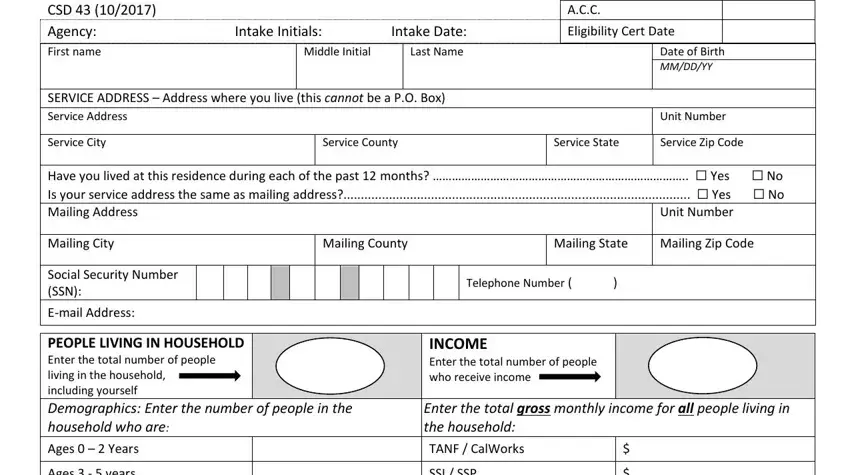
2. Soon after finishing the previous section, head on to the next part and complete the essential particulars in these blank fields - Ages years, Ages years, Ages, Ages and older, Disabled, Native American, Seasonal or Migrant Farmworker, SSI SSP, SSA SSDI, Paychecks, Interest, Pension, Other, Total Monthly Income, and HOUSEHOLD MEMBERS ENTER THE.
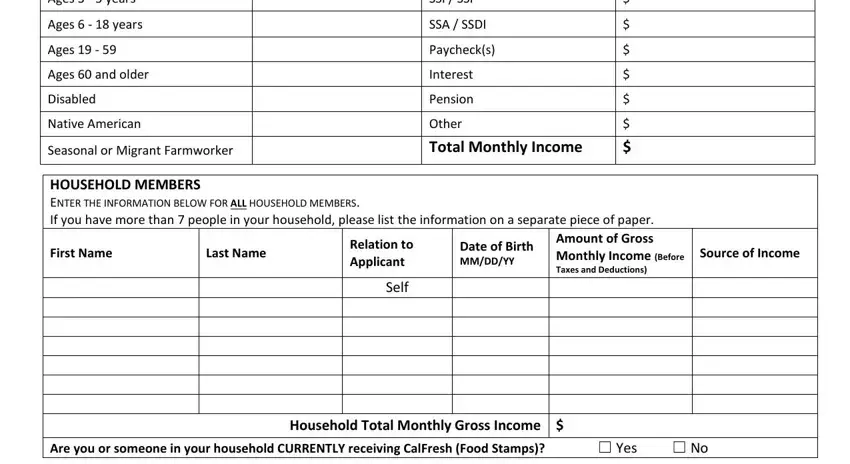
Regarding Ages and older and Seasonal or Migrant Farmworker, be certain that you get them right here. The two of these could be the key fields in this document.
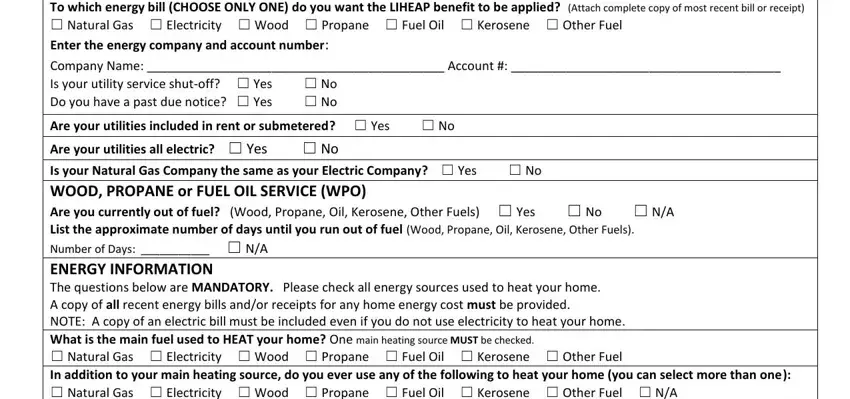
3. The following section will be about PAY BILL To which energy bill, Company Name Account Is your, and Are your utilities included in - type in each one of these blank fields.
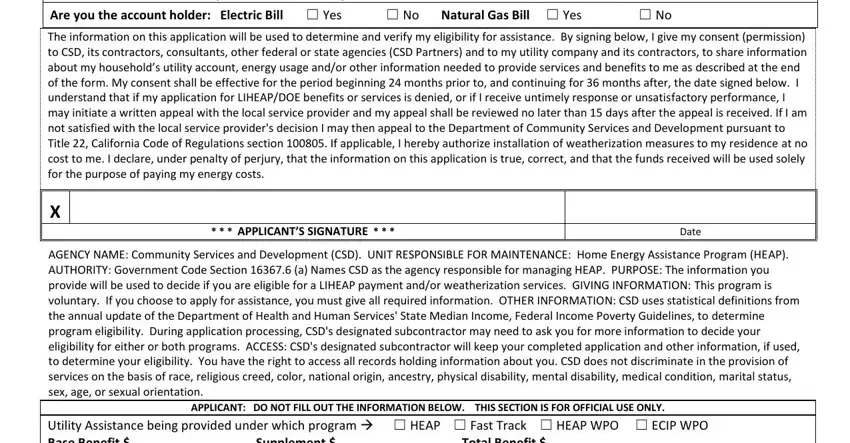
4. The following subsection needs your involvement in the following parts: Are your utilities included in, Are you the account holder, The information on this, APPLICANTS SIGNATURE, Date, AGENCY NAME Community Services and, APPLICANT DO NOT FILL OUT THE, and Utility Assistance being provided. Make certain to give all requested details to go forward.
Step 3: After you have looked once again at the information you filled in, press "Done" to conclude your FormsPal process. Obtain the Csd 43 Form as soon as you register online for a free trial. Conveniently get access to the pdf document within your personal account page, along with any modifications and changes being automatically synced! FormsPal offers risk-free document editor with no personal data record-keeping or distributing. Rest assured that your data is secure here!