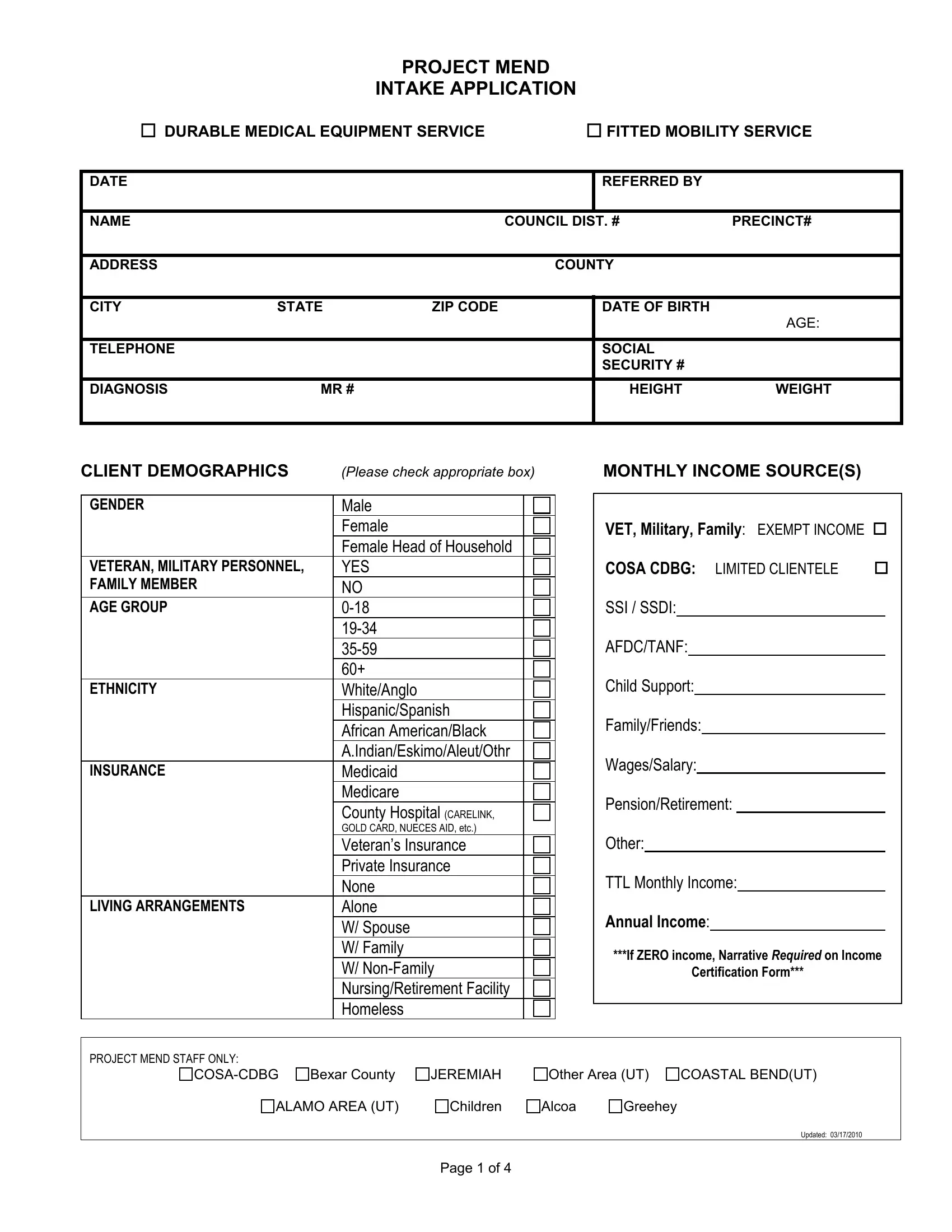
The Project Mend Intake Application form represents a critical step towards securing durable medical equipment and fitted mobility services for individuals in need. Created to ensure that essential equipment reaches those who require assistance for mobility and daily activities, the form carefully gathers detailed information. Starting with basic identification and contact details, it progresses to in-depth queries about the applicant's medical diagnosis, physical characteristics, and demographic information, emphasizing a comprehensive understanding of the applicant's situation. Moreover, it takes into account the applicant’s living arrangements, income sources, and insurance coverage, ensuring a holistic assessment of their circumstances. The form also outlines the terms of the service agreement, highlighting the recipient's responsibilities towards the maintenance and appropriate use of the provided equipment. It incorporates a waiver and release of liability, a media release statement, and income eligibility certification, addressing legal considerations and consent for publicity. Project Mend’s commitment to supporting individuals with mobility challenges is evident in the thoroughness of this application process, aiming to match services and equipment with the needs identified by healthcare professionals.
| Question | Answer |
|---|---|
| Form Name | Project Mend Intake Application Form |
| Form Length | 4 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 1 min |
| Other names | CARELINK, 2009, DME, project mend in san antonio |