The CSD 43 Energy Intake Form is the official document administered by the California Department of Community Services and Development to enroll low-income households in the Home Energy Assistance Program (HEAP). Through HEAP, eligible families and individuals receive financial assistance to pay their energy bills or access weatherization services that reduce long-term energy costs. This energy intake form is the primary application document for Contra Costa County residents and is processed at authorized Community Action Agencies throughout California.
To qualify for HEAP energy assistance through the CSD 43 intake form, your household income must fall at or below 200% of the federal poverty guidelines. Priority consideration goes to households with elderly members age 60 or older, individuals with disabilities, children age 5 and younger, and households facing an imminent utility disconnection. Seasonal and migrant farmworkers, Native American households, and SSI/SSDI recipients also receive priority within the program.
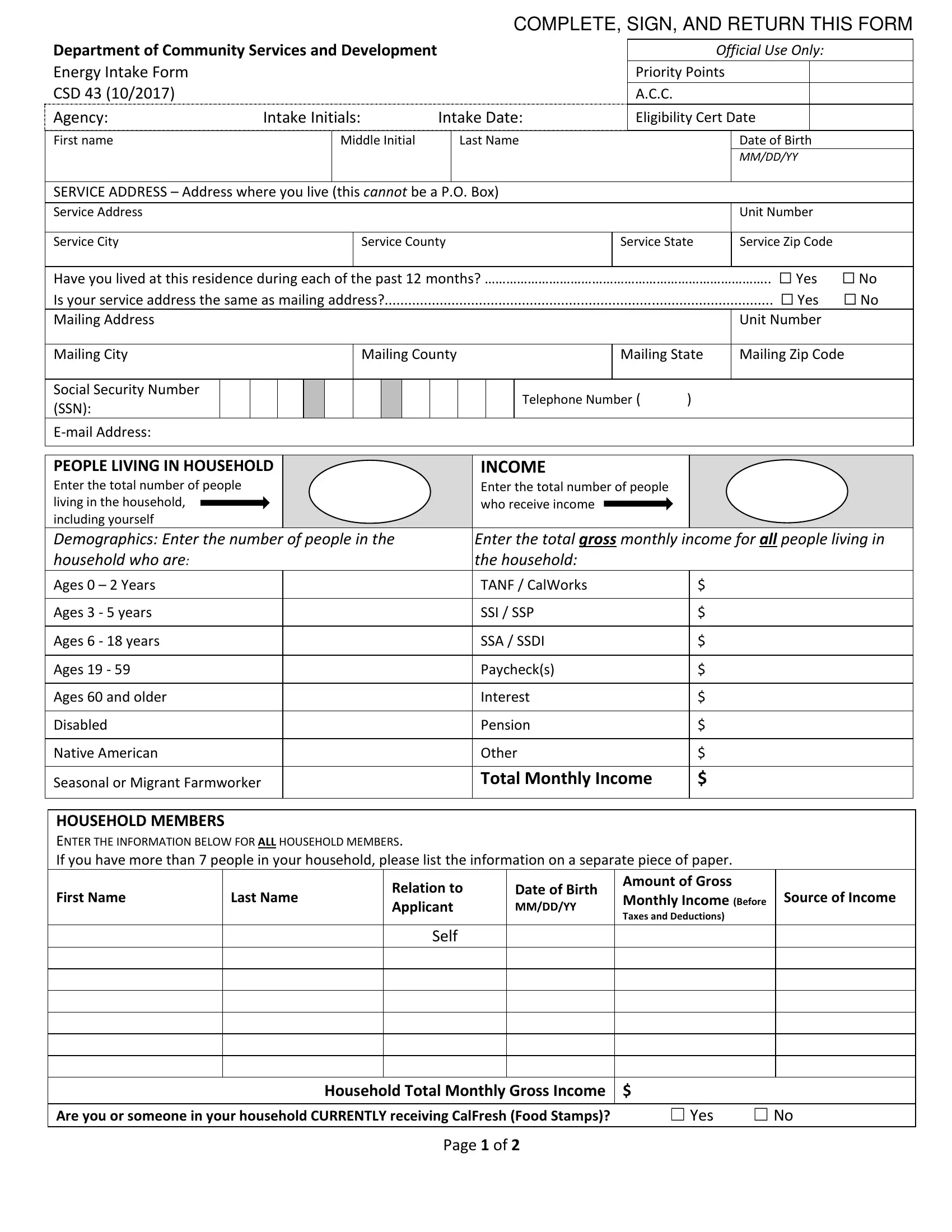
When completing this energy intake form, you will need to provide details about every person in your household, including their ages, disability status, and income sources. Required income documentation covers paychecks, Social Security payments, SSI/SSP benefits, SSDI, pension income, interest income, and any other monthly earnings. The form also asks about the type of energy used in your home, your current utility account status, and whether a disconnection notice is pending.
The CSD 43 form authorizes the sharing of your household information with partner agencies that administer energy programs. After submission, caseworkers review your eligibility and may refer you to either direct financial assistance to pay your energy bills or to weatherization services that improve your home's insulation, heating, and cooling systems. Weatherization improvements are provided at no cost to eligible households and create lasting reductions in monthly energy expenses.
If you need additional forms related to utility or financial assistance, explore our LIHEAP application form, energy low income verification form, and financial assistance application for related programs.
| Question | Answer |
|---|---|
| Form Name | Csd 43 Energy Intake Form |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | form csd xlsm, csd43 form, csd 43 form, 43 energy intake form |