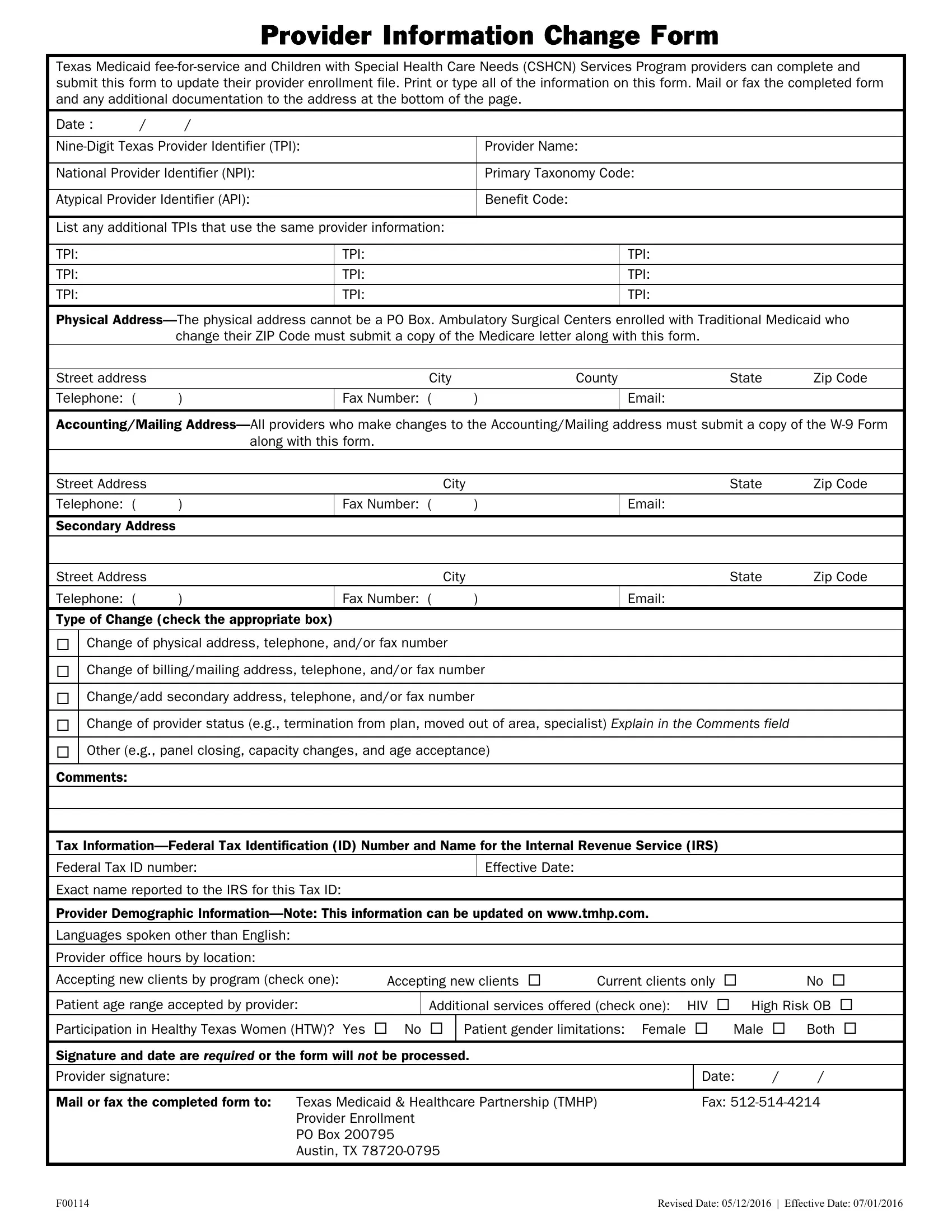
Updating provider information is a critical aspect of maintaining accurate records for Texas Medicaid fee-for-service and the Children with Special Health Care Needs (CSHCN) Services Program. Providers facing changes in their practice, such as changes in physical location, billing addresses, contact information, provider status, or services offered, are required to complete the Provider Information Change Form. This ensures that both the healthcare system and patients have up-to-date information, which is essential for seamless service delivery and billing processes. The form asks for comprehensive details like the nine-digit Texas Provider Identifier (TPI), National Provider Identifier (NPI), Atypical Provider Identifier (API), physical and mailing addresses, as well as tax information. Additionally, to accommodate changes associated with billing or the physical location, supporting documents like the W-9 form or a Medicare letter for certain ZIP code changes are necessitated. Providers can also update demographic information such as languages spoken, office hours, and patient age range accepted. Importantly, a signature is mandatory for the form to be processed, highlighting the importance of the provider's acknowledgment of the accuracy of the submitted information. Mailing or faxing the completed form to the Texas Medicaid & Healthcare Partnership (TMHP) finalizes the process, ensuring the provider's information is up-to-date in the state's health-care system.
| Question | Answer |
|---|---|
| Form Name | Provider Information Change Form |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | form changes medicaid, form tmhp services get, address change tmhp, tmhp |
Provider Information Change Form
Texas Medicaid
Date : |
/ |
/ |
|
|
|
||
Provider Name: |
|||
|
|
||
National Provider Identifier (NPI): |
Primary Taxonomy Code: |
||
|
|
||
Atypical Provider Identifier (API): |
Benefit Code: |
||
|
|
|
|
List any additional TPIs that use the same provider information:
TPI:
TPI:
TPI:
TPI: |
TPI: |
TPI: |
TPI: |
TPI: |
TPI: |
|
|
Physical
Street address |
|
City |
|
County |
State |
Zip Code |
|
|
|
|
|
|
|
Telephone: ( |
) |
Fax Number: ( |
) |
|
Email: |
|
|
|
|
|
|
|
|
Accounting/Mailing
Street Address |
|
|
City |
State |
Zip Code |
|
|
|
|
|
|
Telephone: ( |
) |
Fax Number: ( |
) |
Email: |
|
|
|
|
|
|
|
Secondary Address |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Street Address |
|
|
City |
State |
Zip Code |
Telephone: ( |
) |
Fax Number: ( |
) |
Email: |
|
Type of Change (check the appropriate box)
Change of physical address, telephone, and/or fax number
Change of billing/mailing address, telephone, and/or fax number
Change/add secondary address, telephone, and/or fax number
Change of provider status (e.g., termination from plan, moved out of area, specialist) Explain in the Comments field
Other (e.g., panel closing, capacity changes, and age acceptance)
Comments:
Tax
Federal Tax ID number: |
Effective Date: |
Exact name reported to the IRS for this Tax ID:
Provider Demographic
Languages spoken other than English:
Provider office hours by location:
Accepting new clients by program (check one): |
Accepting new clients |
Current clients only |
|
|
No |
|||||
Patient age range accepted by provider: |
|
Additional services offered (check one): |
HIV |
|
High Risk OB |
|
||||
Participation in Healthy Texas Women (HTW)? Yes |
No |
Patient gender limitations: Female |
|
|
Male |
Both |
|
|||
|
|
|
|
|
|
|
|
|
||
Signature and date are required or the form will not be processed. |
|
|
|
|
|
|
|
|||
Provider signature: |
|
|
|
|
|
Date: |
/ |
/ |
|
|
|
|
|
|
|||||||
Mail or fax the completed form to: Texas Medicaid & Healthcare Partnership (TMHP) |
|
Fax: |
|
|||||||
Provider Enrollment |
|
|
|
|
|
|
|
|||
PO Box 200795 |
|
|
|
|
|
|
|
|||
Austin, TX |
|
|
|
|
|
|
|
|||
F00114 |
REVISED DATE: 05/12/2016 | EFFECTIVE DATE: 07/01/2016 |
Instructions for Completing the
Provider Information Change Form
Signatures
•The provider’s signature is required on the Provider Information Change Form for any and all changes requested for individual provider numbers.
•A signature by the authorized representative of a group or facility is acceptable for requested changes to group or facility provider numbers.
Address
•Performing providers (physicians performing services within a group) may not change accounting information.
•For Texas Medicaid
•For Texas Medicaid
Federal Tax Identification Number (TIN)
•Federal TIN changes for individual practitioner provider numbers can only be made by the individual to whom the number is assigned.
•Performing providers cannot change the Federal TIN.
Provider Demographic Information
An online provider lookup (OPL) is available, which allows users such as clients and providers to view information about Texas State
General
•TMHP must have either the
•The
•Mail or fax the completed form to:
Texas Medicaid & Healthcare Partnership (TMHP)
Provider Enrollment
PO Box 200795
Austin, TX
Fax:
F00114 |
REVISED DATE: 05/12/2016 | EFFECTIVE DATE: 07/01/2016 |