
With the help of the online tool for PDF editing by FormsPal, it is possible to fill out or modify saha change of income form right here. In order to make our editor better and easier to work with, we constantly work on new features, taking into consideration feedback from our users. Starting is effortless! All you should do is follow these simple steps directly below:
Step 1: Press the "Get Form" button at the top of this page to open our tool.
Step 2: The tool gives you the capability to modify almost all PDF files in a range of ways. Change it by adding customized text, adjust what's already in the PDF, and place in a signature - all within a couple of clicks!
In an effort to complete this document, be sure to enter the information you need in every single blank field:
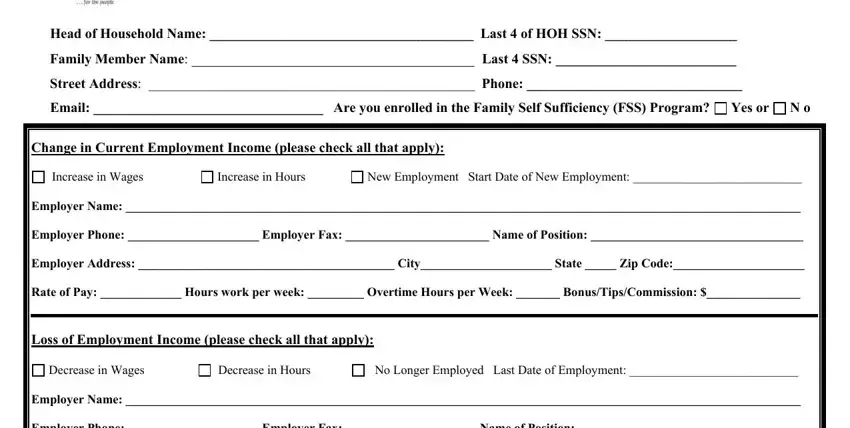
1. The saha change of income form needs specific information to be typed in. Be sure the subsequent blanks are complete:
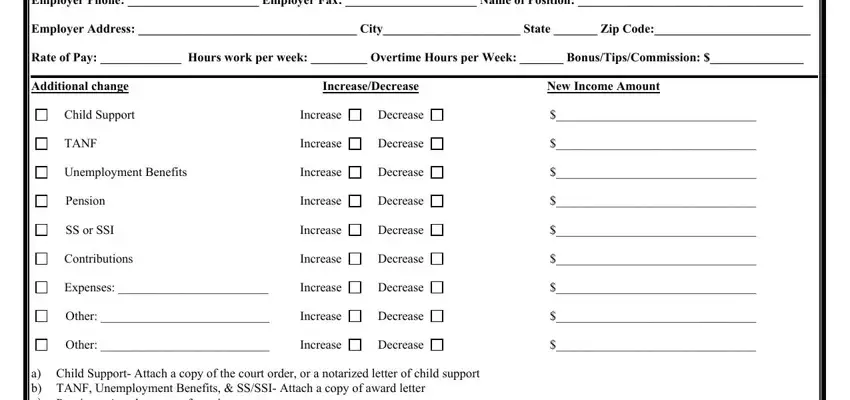
2. Once your current task is complete, take the next step – fill out all of these fields - TANF, Child Support, Decrease, Increase, Decrease, Unemployment Benefits, Employer Name Employer Phone, Expenses, Other, Other, Increase, Decrease, Increase, Decrease, and Decrease with their corresponding information. Make sure to double check that everything has been entered correctly before continuing!
3. This subsequent part should also be quite easy, Name, Address, Last of SSN, City, State, Zip, Phone Number, Email Address, and Statement Please Print - all these fields is required to be filled in here.
4. Completing Warning USC provides that, By signing below I am certifying, Signature, In the presence of Signature, Date, and Any individual with a disability is crucial in the next form section - ensure that you devote some time and be mindful with each and every empty field!
5. Lastly, the following last subsection is precisely what you'll have to complete prior to submitting the form. The fields you're looking at are the following: Authorization for the Release of, IHA requesting release of, Authority Section of the Stewart, This law requires that you sign a, Persons who apply for or receive, PHAowned rental public housing, Turnkey III Homeownership, Mutual Help Homeownership, Section and c leased housing, Section Housing Assistance, HAowned rental Indian housing, and Section Rental Certificate.
Always be really careful when filling out Turnkey III Homeownership and Section Rental Certificate, since this is the section in which many people make mistakes.
Step 3: Look through the details you have inserted in the blank fields and then click on the "Done" button. Go for a 7-day free trial account at FormsPal and gain immediate access to saha change of income form - downloadable, emailable, and editable inside your personal account page. We don't share any information you type in whenever filling out forms at FormsPal.