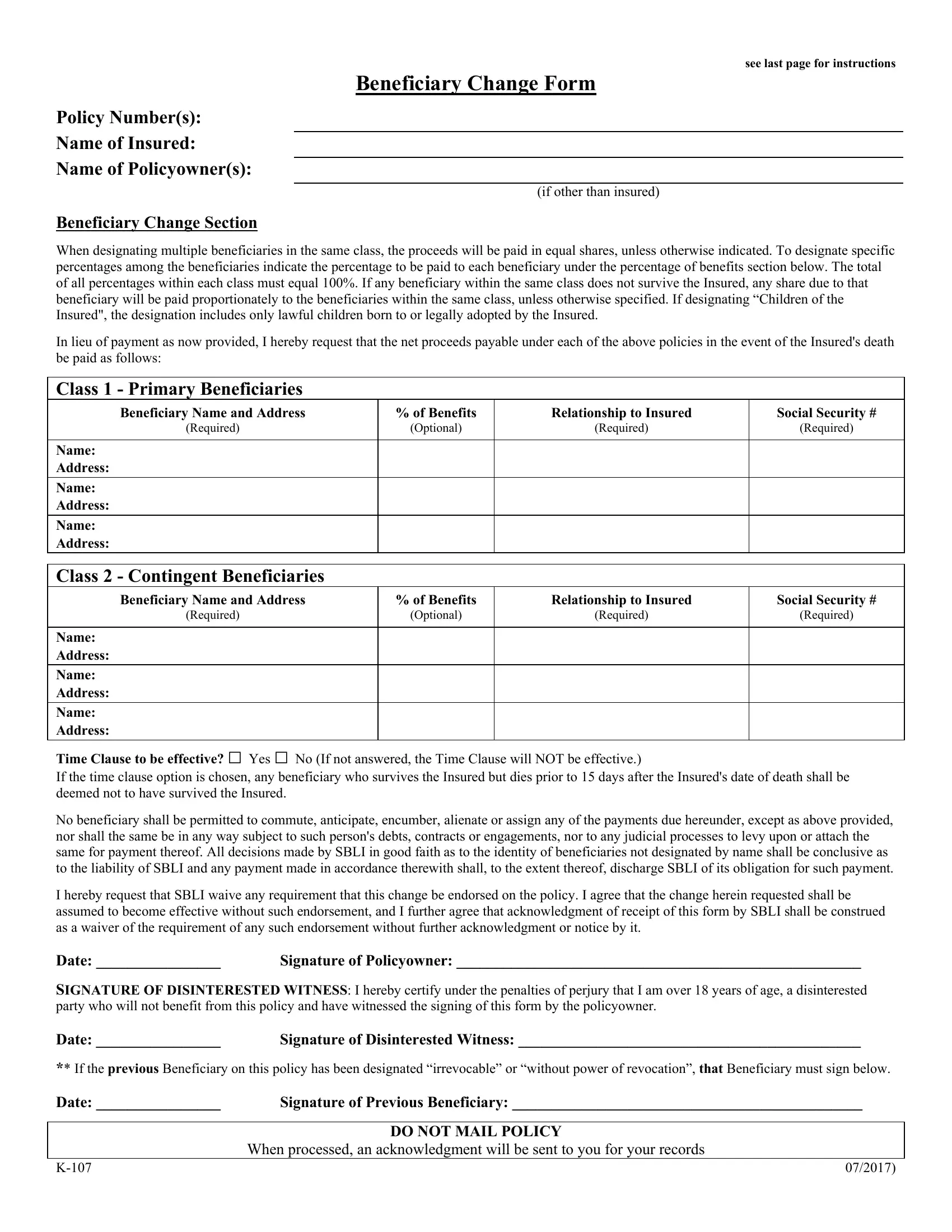
Navigating through the requirements of updating your life insurance policy can often feel daunting, especially when it comes to something as crucial as changing beneficiaries. The SBLI (Savings Bank Life Insurance) Change Form is designed to facilitate this exact process, allowing policy owners to adjust their primary and contingent beneficiaries with ease. This document covers essential details such as policy number, insured and policy owner names, and provides a structured way to designate or modify beneficiaries across two primary classes. It permits the allocation of specific percentages of benefits to each, ensuring the policy proceeds are distributed according to the policy owner's wishes. Further, it introduces the concept of a time clause to manage the succession of beneficiaries under particular circumstances, alongside stipulating requirements for the provision of beneficiary information such as addresses and social security numbers. Completing and submitting this form correctly is crucial, as it replaces any prior beneficiary designations on the record and can significantly influence the financial future of the designated individuals or entities. This introduction serves to pinpoint the critical components and provide guidance on how to accurately execute a beneficiary change, ensuring the policy benefits are aligned with the current intentions of the policy owner.
| Question | Answer |
|---|---|
| Form Name | Sbli Change Form |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | sbli beneficiary change form, sbli change online, sbli life insurance change of beneficiary, sbli forms |