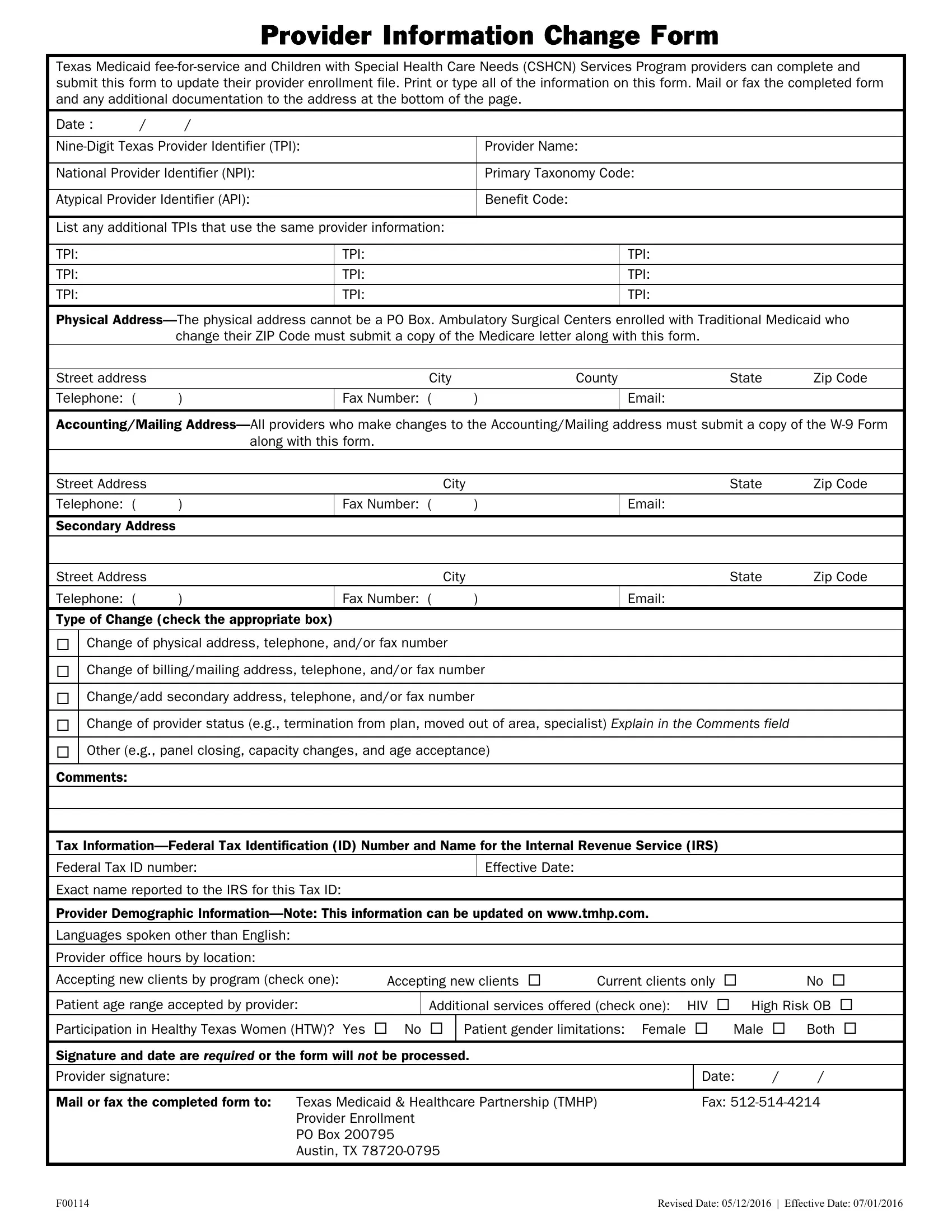
Updating provider information is a critical aspect of maintaining accurate records for Texas Medicaid fee-for-service and the Children with Special Health Care Needs (CSHCN) Services Program. Providers facing changes in their practice, such as changes in physical location, billing addresses, contact information, provider status, or services offered, are required to complete the Provider Information Change Form. This ensures that both the healthcare system and patients have up-to-date information, which is essential for seamless service delivery and billing processes. The form asks for comprehensive details like the nine-digit Texas Provider Identifier (TPI), National Provider Identifier (NPI), Atypical Provider Identifier (API), physical and mailing addresses, as well as tax information. Additionally, to accommodate changes associated with billing or the physical location, supporting documents like the W-9 form or a Medicare letter for certain ZIP code changes are necessitated. Providers can also update demographic information such as languages spoken, office hours, and patient age range accepted. Importantly, a signature is mandatory for the form to be processed, highlighting the importance of the provider's acknowledgment of the accuracy of the submitted information. Mailing or faxing the completed form to the Texas Medicaid & Healthcare Partnership (TMHP) finalizes the process, ensuring the provider's information is up-to-date in the state's health-care system.
| Question | Answer |
|---|---|
| Form Name | Provider Information Change Form |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | form changes medicaid, form tmhp services get, address change tmhp, tmhp |
