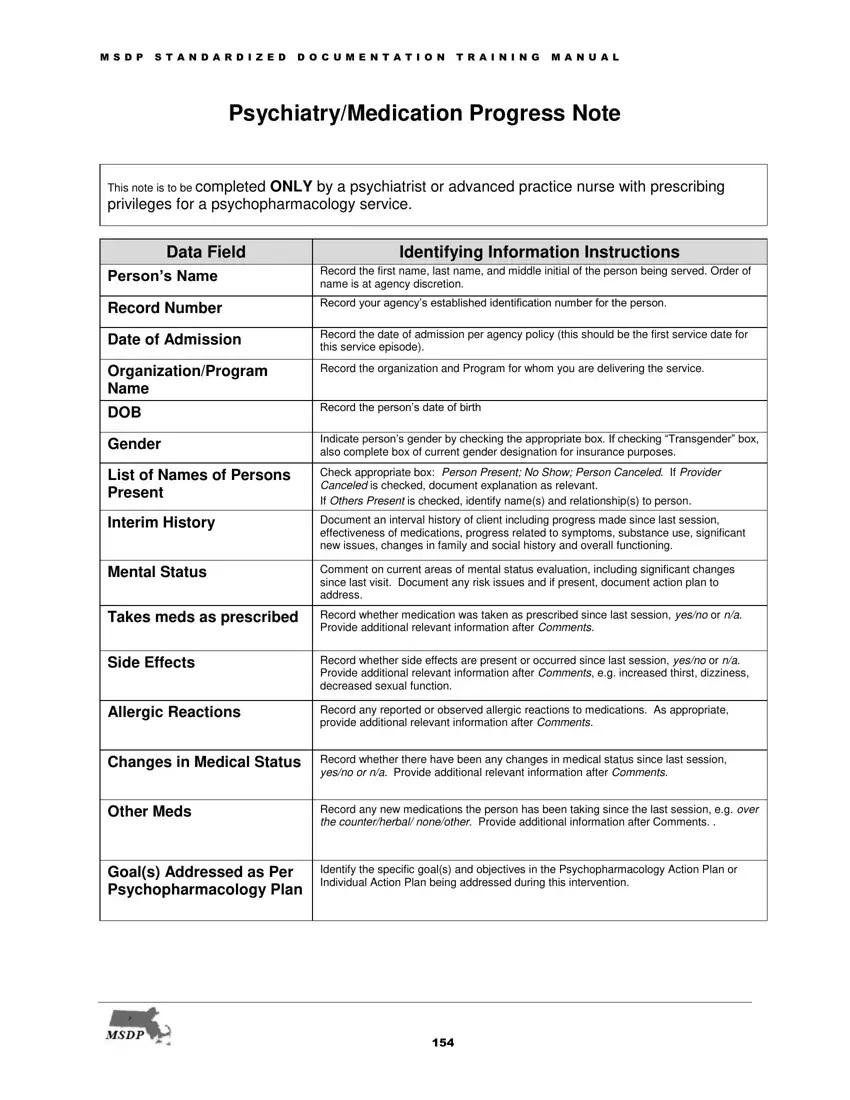
In the realm of psychiatric care, maintaining accurate and thorough documentation is not just a procedural necessity but also a cornerstone of effective treatment planning and patient safety. The Psychiatric Progress Note form, designed exclusively for use by psychiatrists or advanced practice nurses with prescribing privileges in a psychopharmacology service, embodies this principle. This detailed form covers several crucial areas of patient care, including identifying information, interim history, mental status, medication adherence, side effects, allergic reactions, changes in medical status, and more. It ensures the systematic tracking of a patient's progress, response to medication, and any modification in treatment strategy, thereby playing a pivotal role in the continuum of care. By documenting therapeutic interventions—from psychotherapy to medication management—and summarizing laboratory test results, the form facilitates a comprehensive review of the patient's journey. Moreover, the emphasis on informed consent and detailed instructions underscores the commitment to patient autonomy and education. This precise approach to documentation not only aids in monitoring the efficacy of interventions but also ensures a high standard of care through clear communication and accountability.
| Question | Answer |
|---|---|
| Form Name | Psychiatric Progress Note |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | psychiatric progress note pdf, outpatient psychiatry note template, psychiatric documentation templates, psychiatry note template |
