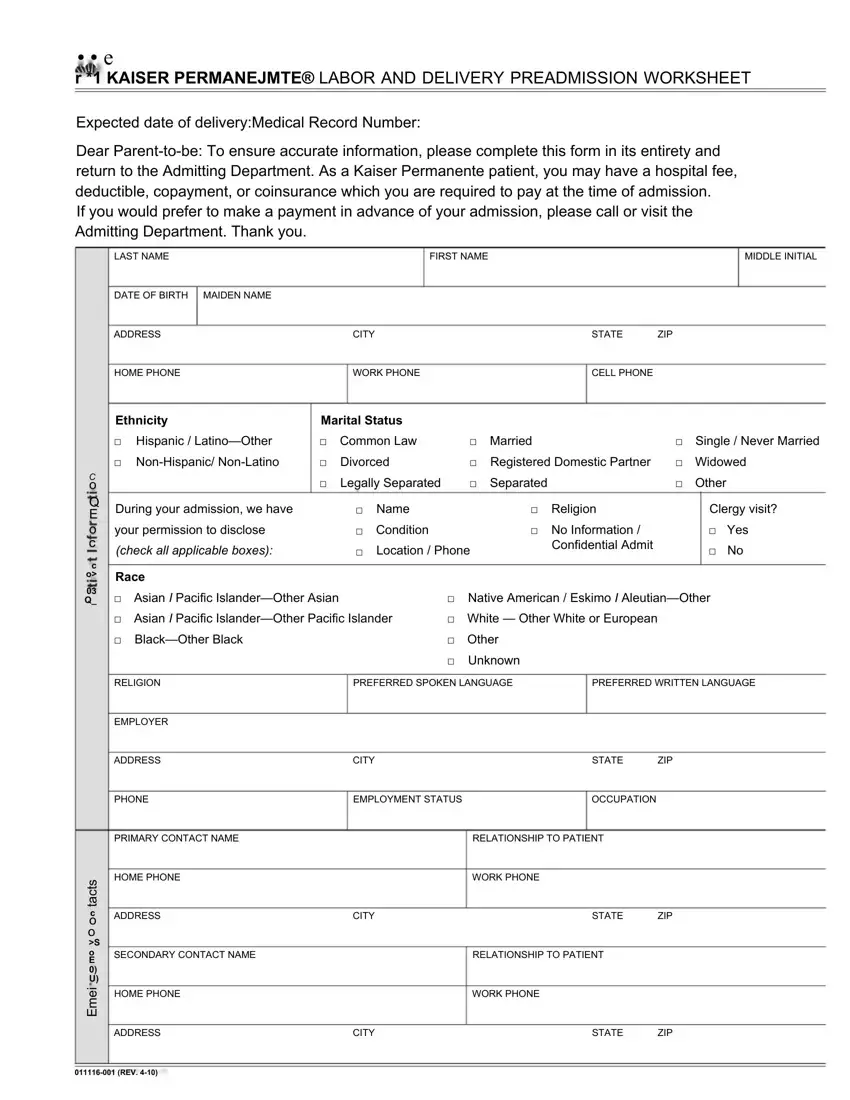
Navigating the preparation for labor and delivery involves several crucial steps, among which filling out the Kaiser Work Note form, specifically designed as a labor and delivery preadmission worksheet, stands out. This comprehensive document serves an array of purposes, primary among them being the facilitation of a smooth admission process for expectant parents under the Kaiser Permanente healthcare umbrella. It requires detailed personal information, including expected delivery date, medical record number, demographic details, and contact information, which ensures that the hospital can provide tailored care according to the patient's medical and personal needs. Additionally, it outlines financial obligations such as hospital fees, deductibles, copayments, or coinsurance, providing an option for preadmission payments to ease the process. Furthermore, the form requests specifics on the newborn's information, advance directive information, and subscriber details to ensure that the hospital staff has all necessary information at their fingertips. By meticulously completing this worksheet and returning it to the Admitting Department, expectant parents can look forward to a more organized and less stressful admission process, paving the way for a focus on the joyous occasion of welcoming a new life.
| Question | Answer |
|---|---|
| Form Name | Kaiser Work Note |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | kaiser doctors note for work, printable kaiser doctors note pdf, doctors note kaiser, kaiser doctors note pdf |
