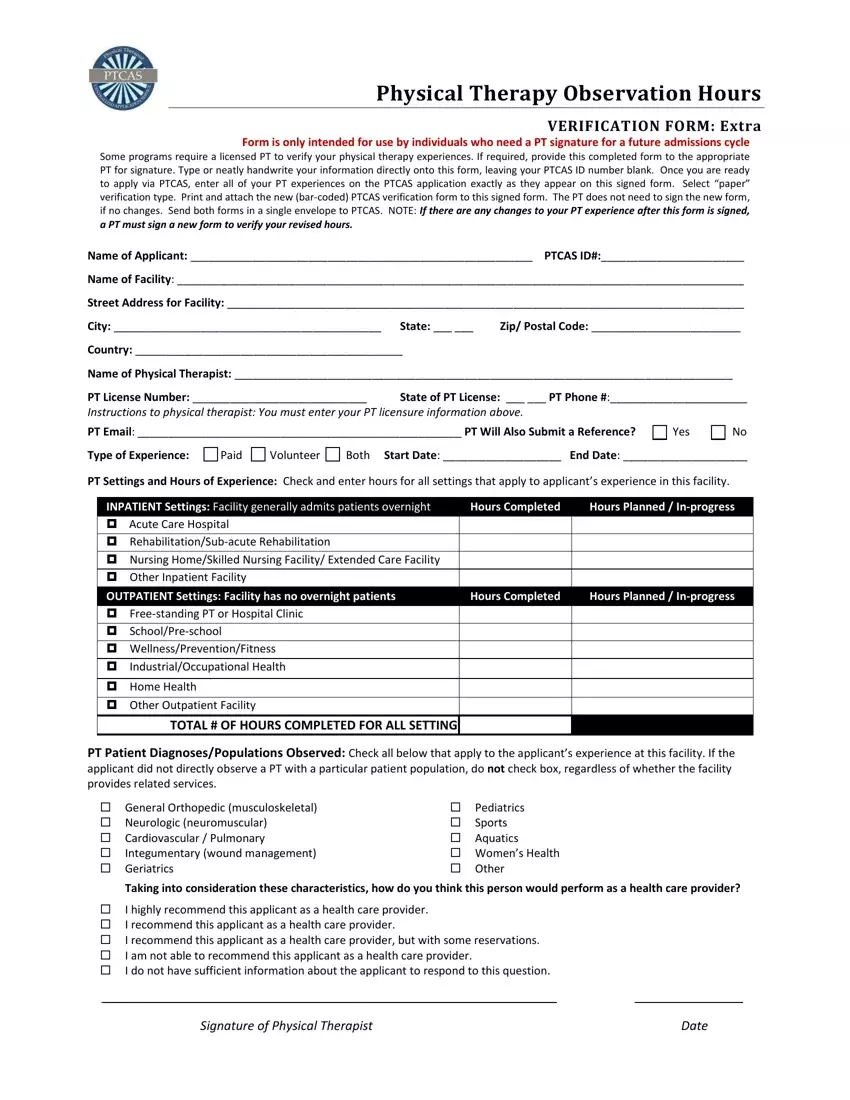
The pursuit of a career in physical therapy demands rigorous preparation, part of which involves accumulating relevant experience in various settings. For individuals targeting admission into physical therapy programs, the Physical Therapy Centralized Application Service (PTCAS) form plays a pivotal role in this process. Specifically designed for those who need to have their physical therapy observation hours verified by a licensed physical therapist, the Physical Therapy Observation Hours Verification Form is a crucial document. It requires detailed input from applicants regarding their experiences across different settings, including both inpatient and outpatient facilities. The form not only captures the duration and nature of these experiences—categorizing them as paid, volunteer, or both—but also the types of patient diagnoses and populations observed. Critical instructions guide both the applicant and the verifying physical therapist on how to accurately complete and submit the form. Additionally, the document offers a section for the physical therapist to endorse the applicant's potential as a healthcare provider. This endorsement can significantly influence admissions decisions, making the accurate and thorough completion of this form essential for prospective physical therapy students. This process underscores the importance of comprehensive and verifiable hands-on experience in the highly competitive field of physical therapy.
| Question | Answer |
|---|---|
| Form Name | Ptcas Form |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | observation hours form, therapy observation form, paper form for physical therapy observation hours, ptcas observation hours verification form |
