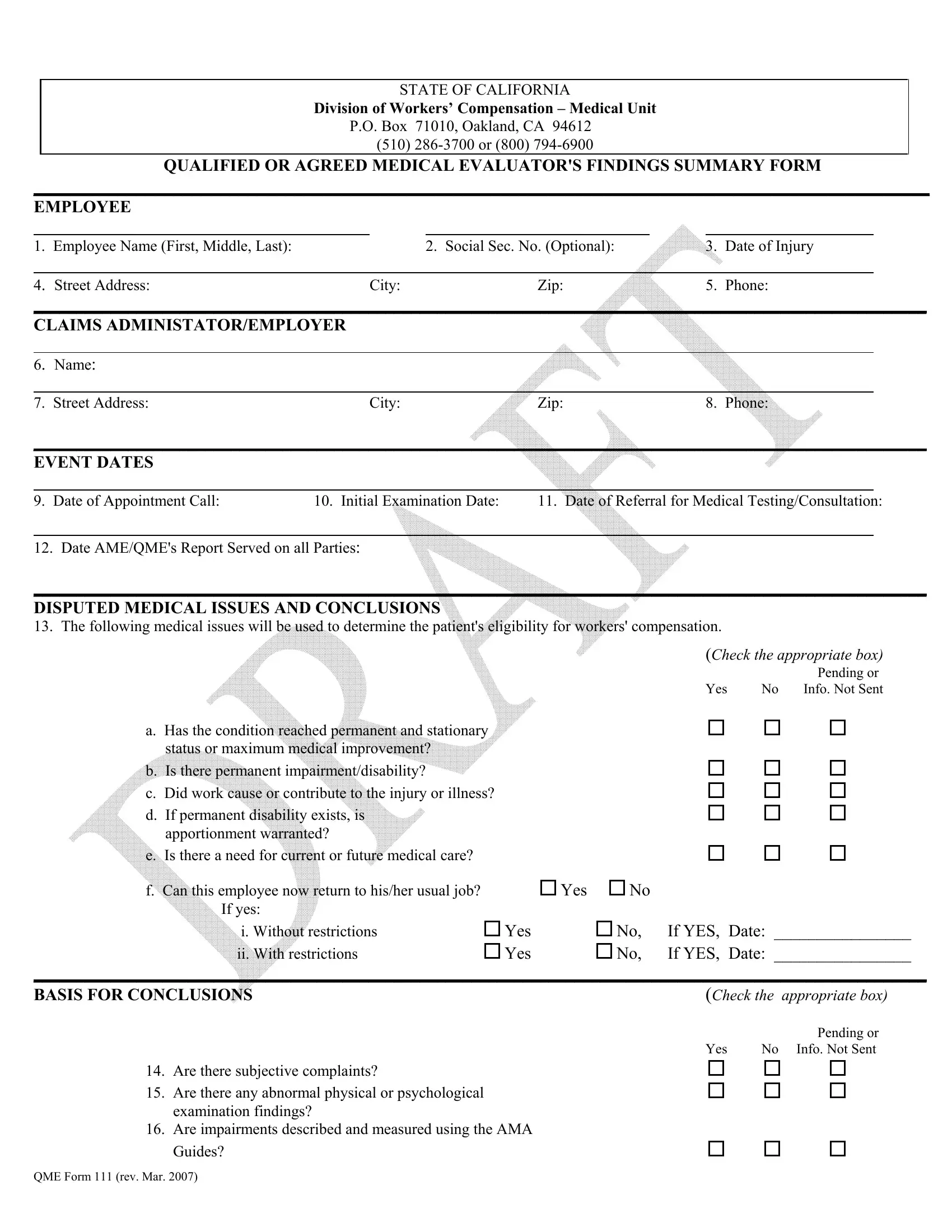
The QME 111 form, an essential document within the California workers' compensation system, outlines the findings of a Qualified or Agreed Medical Evaluator regarding an employee's work-related injury or illness. This comprehensive form, curated by the State of California Division of Workers’ Compensation – Medical Unit, serves as a critical communication tool between medical evaluators, employees, and claims administrators or employers. It meticulously captures a range of details including personal information about the employee, specifics about the claims administrator or employer, crucial event dates like the appointment call and initial examination, along with disputed medical issues and the evaluator’s conclusions. Additionally, it is instrumental in documenting the process of medical evaluation through listings of subjective complaints, abnormal findings, diagnostic test results, and the crucial utilization of the AMA Guides for determining impairment. The form also details the review of medical records and consultations with other physicians, culminating in the QME or AME's signed declaration. Satisfying legal requirements, this form is designed to ensure clear, concise, and transparent communication of an employee's medical evaluation findings, facilitating the determination of eligibility for workers' compensation benefits. By providing a structured summary of the evaluator's findings, it supports the fair and efficient resolution of workers' compensation claims, making it a pivotal document for all parties involved in the adjudication process.
| Question | Answer |
|---|---|
| Form Name | Qme Form 111 |
| Form Length | 3 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 45 sec |
| Other names | thereon, DEU, ADMINISTATOR, qualified or agreed medical evaluator's findings summary form fill in |
