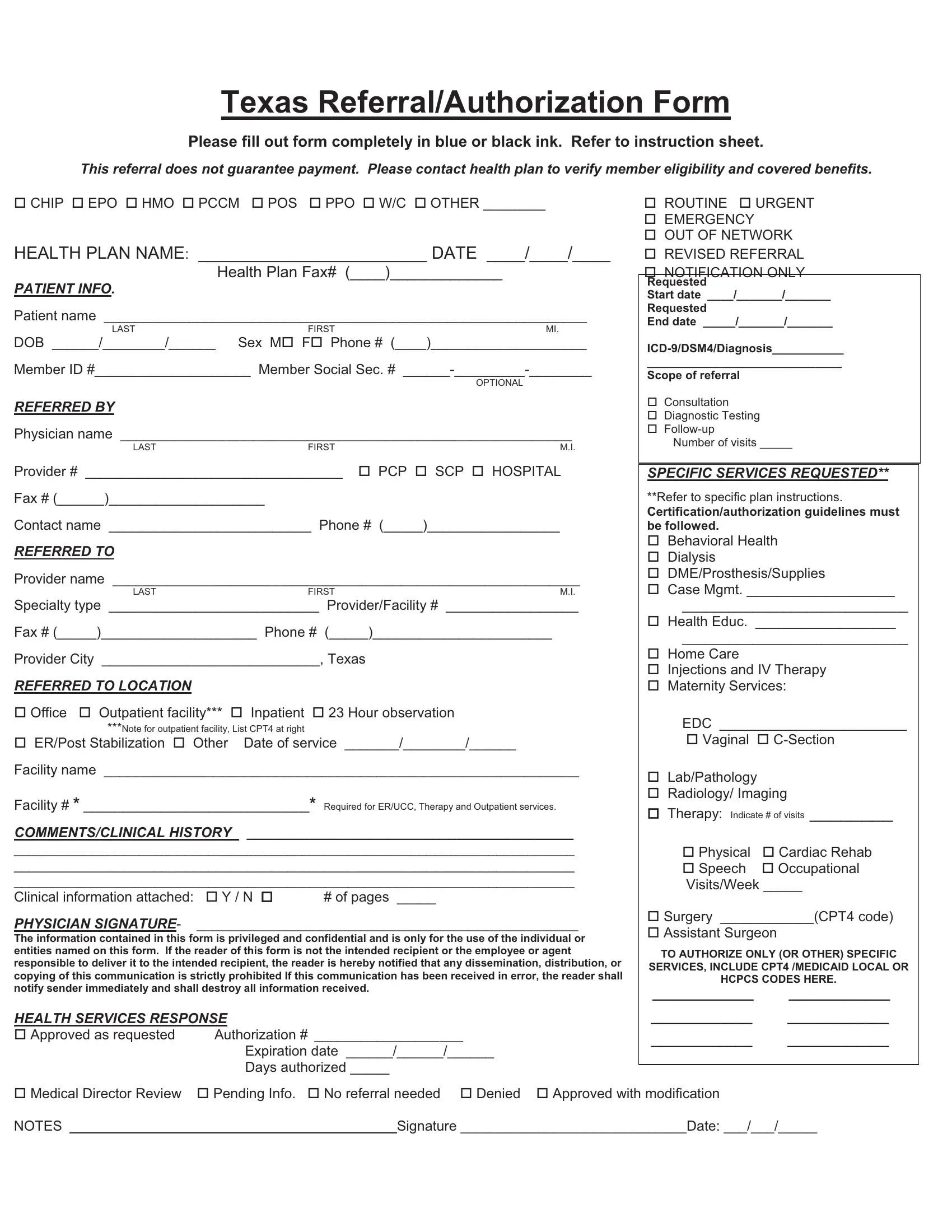
In navigating the complexities of healthcare coverage, the Texas Referral/Authorization Form emerges as a crucial document for both patients and healthcare providers. This comprehensive form, to be filled out with precise attention using blue or black ink, guides the submission process for varying types of healthcare plans, including but not limited to CHIP, EPO, HMO, PCCM, POS, PPO, and others. It mandates the submission of detailed patient information, referral sources, and targeted provider details, aiming to streamline the communication between healthcare entities and insurance plans. By instructing users to verify member eligibility and benefit coverage with their respective health plans, it underscores the reality that a referral does not inherently guarantee payment. Alongside capturing essential data — like patient demographics, referring and referred to provider information, and service specifications — this form also makes room for comments on clinical history and the attaching of pertinent clinical documents. Its segments on health services response highlight the sense of urgency and the scope of the referral, ranging from routine to emergency, and clarifies the process for approval or denial. This all-encompassing approach not only aids in the effective referral of patients within Texas but also emphasizes the importance of detailed communications and adherence to specific plan instructions for successful healthcare service authorization.
| Question | Answer |
|---|---|
| Form Name | Referral Authorization Form |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | outside referral form parkland hospital, parklabd referral form, parkland referrals, parkland outside referral form |
Texas Referral/Authorization Form
Please fill out form completely in blue or black ink. Refer to instruction sheet.
This referral does not guarantee payment. Please contact health plan to verify member eligibility and covered benefits.
CHIP EPO HMO PCCM POS PPO W/C OTHER ________
HEALTH PLAN NAME: ________________________ DATE ____/____/____
Health Plan Fax# (____)_____________
PATIENT INFO.
Patient name ______________________________________________________________
LAST |
FIRST |
MI. |
DOB ______/________/______ |
Sex M F Phone # (____)____________________ |
|
Member ID #____________________ Member Social Sec. #
OPTIONAL
REFERRED BY
Physician name __________________________________________________________
LAST |
FIRST |
|
|
M.I. |
Provider # _________________________________ |
PCP |
SCP |
HOSPITAL |
|
Fax # (______)____________________ |
|
|
|
|
Contact name __________________________ Phone # (_____)_________________
REFERRED TO
Provider name ____________________________________________________________
|
LAST |
|
FIRST |
M.I. |
|
Specialty type ___________________________ |
Provider/Facility # |
_________________ |
|||
Fax # (_____)____________________ Phone # (_____)_______________________ |
|||||
Provider City ____________________________, Texas |
|
||||
REFERRED TO LOCATION |
|
|
|
|
|
Office |
Outpatient facility*** |
Inpatient |
23 Hour observation |
||
|
***Note for outpatient facility, List CPT4 at right |
|
|
||
ER/Post Stabilization |
Other |
Date of service _______/________/______ |
|||
Facility name _____________________________________________________________
Facility # * _____________________________* Required for ER/UCC, Therapy and Outpatient services.
COMMENTS/CLINICAL HISTORY __________________________________________
________________________________________________________________________
________________________________________________________________________
________________________________________________________________________
Clinical information attached: |
Y / N |
# of pages _____ |
PHYSICIAN SIGNATURE- |
_________________________________________________ |
|
The information contained in this form is privileged and confidential and is only for the use of the individual or entities named on this form. If the reader of this form is not the intended recipient or the employee or agent responsible to deliver it to the intended recipient, the reader is hereby notified that any dissemination, distribution, or copying of this communication is strictly prohibited If this communication has been received in error, the reader shall notify sender immediately and shall destroy all information received.
HEALTH SERVICES RESPONSE
Approved as requested |
Authorization # ___________________ |
|
Expiration date ______/______/______ |
|
Days authorized _____ |
ROUTINE URGENT
EMERGENCY
OUT OF NETWORK
REVISED REFERRAL
NOTIFICATION ONLY
Requested
Start date ____/_______/_______
Requested
End date _____/_______/_______
______________________________
Scope of referral
Consultation
Diagnostic Testing
Number of visits _____
SPECIFIC SERVICES REQUESTED**
**Refer to specific plan instructions.
Certification/authorization guidelines must be followed.
Behavioral Health Dialysis DME/Prosthesis/Supplies
Case Mgmt. ___________________
_____________________________
Health Educ. __________________
_____________________________
Home Care
Injections and IV Therapy Maternity Services:
EDC ________________________
Vaginal
Lab/Pathology
Radiology/ Imaging
Therapy: Indicate # of visits ________
Physical |
Cardiac Rehab |
Speech |
Occupational |
Visits/Week _____
Surgery ____________(CPT4 code)
Assistant Surgeon
TO AUTHORIZE ONLY (OR OTHER) SPECIFIC SERVICES, INCLUDE CPT4 /MEDICAID LOCAL OR HCPCS CODES HERE.
_____________ _____________
_____________ _____________
_____________ _____________
Medical Director Review Pending Info. No referral needed Denied Approved with modification
NOTES __________________________________________Signature _____________________________Date: ___/___/_____