


Handling PDF files online is definitely very easy with our PDF tool. Anyone can fill in register of facility clients residents form here in a matter of minutes. We at FormsPal are dedicated to providing you the best possible experience with our editor by regularly presenting new features and improvements. With these updates, using our editor gets better than ever before! Starting is simple! All that you should do is adhere to the following easy steps down below:
Step 1: Click the orange "Get Form" button above. It is going to open our pdf editor so that you can start completing your form.
Step 2: With our online PDF editing tool, you are able to accomplish more than just fill out blanks. Edit away and make your forms seem sublime with customized text incorporated, or adjust the file's original input to excellence - all supported by the capability to add your personal graphics and sign the document off.
It is straightforward to finish the pdf using this helpful tutorial! Here's what you want to do:
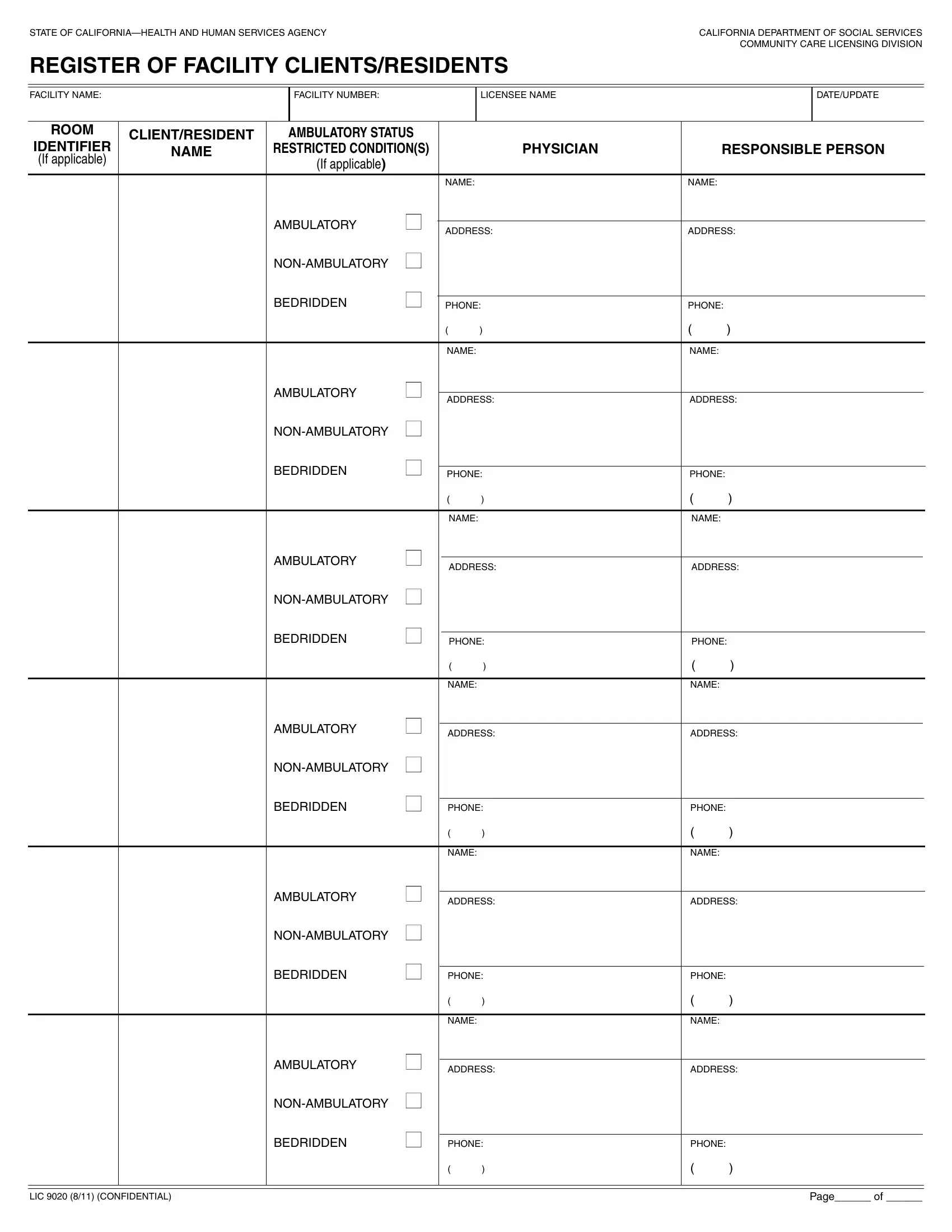
1. Begin filling out the register of facility clients residents form with a number of major fields. Get all the information you need and ensure there is nothing overlooked!
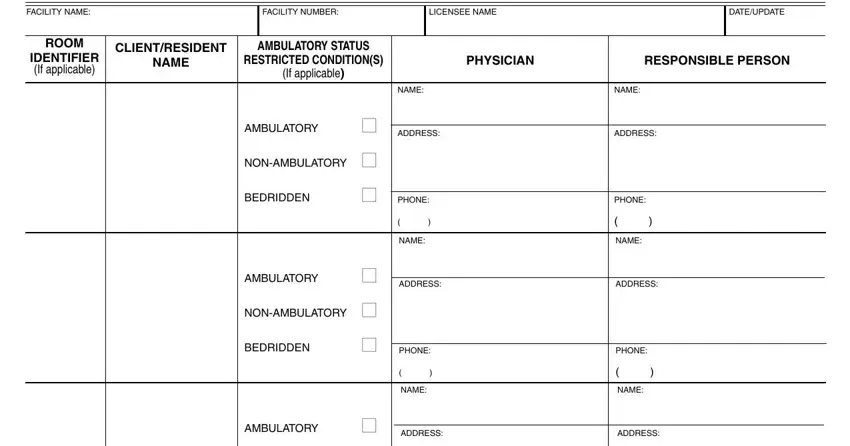
2. The third part is usually to complete the next few blanks: PHONE, NAME, ADDRESS, PHONE, NAME, ADDRESS, PHONE, NAME, ADDRESS, NONAMBULATORY, BEDRIDDEN, PHONE, NAME, AMBULATORY, and ADDRESS.
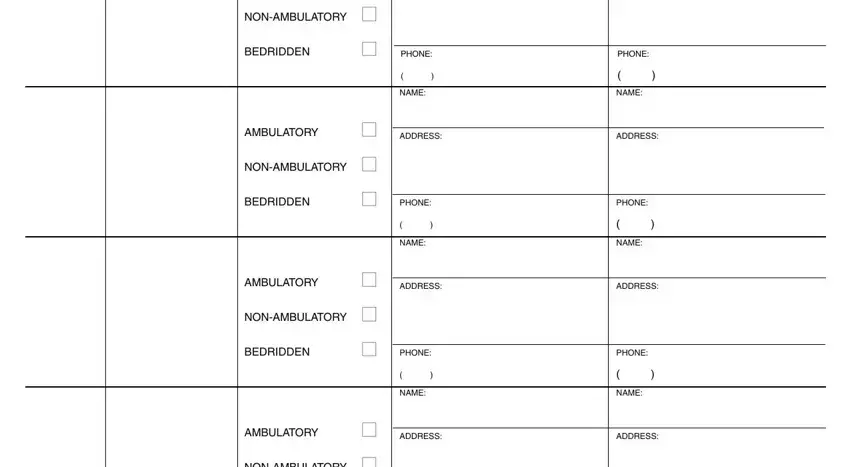
3. Completing PHONE, NONAMBULATORY, BEDRIDDEN, PHONE, LIC CONFIDENTIAL, and Page of is essential for the next step, make sure to fill them out in their entirety. Don't miss any details!

Concerning PHONE and BEDRIDDEN, ensure that you don't make any mistakes in this current part. These two could be the most important ones in the document.
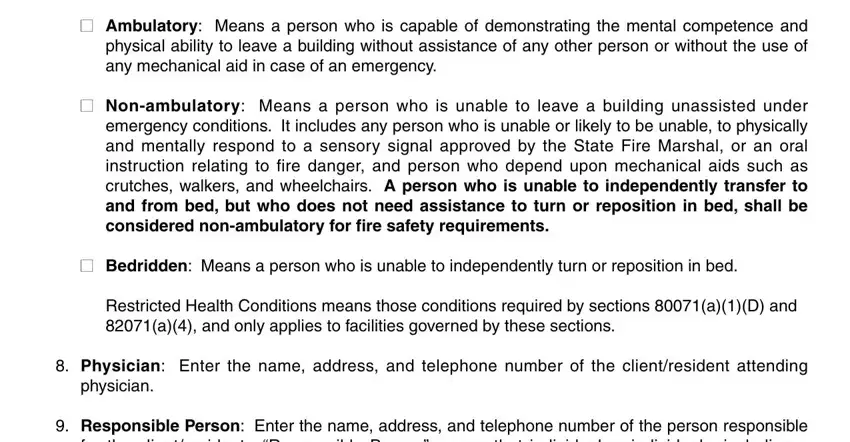
4. Your next subsection requires your details in the following areas: Ambulatory Means a person who is, Nonambulatory Means a person who, Bedridden Means a person who is, Restricted Health Conditions means, Physician Enter the name address, physician, and Responsible Person Enter the name. Be sure to give all needed info to move onward.
5. To finish your document, this particular segment requires several extra blank fields. Filling in LIC CONFIDENTIAL, and Page of will certainly conclude everything and you'll certainly be done very quickly!

Step 3: When you've looked over the information you filled in, press "Done" to finalize your FormsPal process. Make a 7-day free trial account with us and get instant access to register of facility clients residents form - with all transformations preserved and available from your FormsPal account. Here at FormsPal.com, we aim to be sure that all your information is stored secure.