Patient Authorization (PA)
Patients must read this and sign the acknowledgment on the previous page before they can participate in the Program.
My signature on the previous page of this form confirms that I allow my doctor(s), any other healthcare providers, specialty pharmacy providers, and my health plan or insurers to share medical information relating to my use or potential use of REMICADE® (infliximab) with Janssen Biotech, Inc., including our affiliates and our service providers that work on their behalf, in connection with the Program (the ”Companies”).
The Companies administer AccessOne® and RemiStart® (the “Program”) for Janssen Biotech, Inc., maker of REMICADE®.
This information can include spoken or written facts about my health and payment benefits I may have. It may include copies of records from my healthcare providers or health plans about my health or health care.
The Companies may use and share this information to help find alternate funding sources for REMICADE®, and perform other related services. The Companies may also share my information with other related parties of this program or as otherwise set forth above.
The Companies will use and share this information to see if I qualify for the Programs and to run the Programs. In addition, the Companies may use and share my information to refer me to other programs, foundations, or alternate sources of funding or coverage that may be available to provide assistance to me with costs of my medication. Program management employees of the Companies may also see my information, but they may use it only in connection with the Program, to help me get assistance with the costs of my medication, or as otherwise required or allowed under the law. I understand that they will make every effort to keep my information private, but if it is accidentally shared with an associated party, federal privacy laws will not protect it.
This Authorization will last until I am no longer participating in the Program. If I change my mind, I can inform my healthcare providers and my insurers in writing that I do not want them to share any information with AccessOne® and RemiStart® (Janssen Biotech, Inc., including our affiliates and our service providers that work on their behalf, in connection with the Program), but will not change any information shared before I notified them of my desire to discontinue. I know that I have a right to see or copy the information my healthcare providers or insurers have given to the Companies.
I understand that I am not required to sign this form on the previous page. My choice about whether to sign this form will not change the way my healthcare providers or insurers treat me. If I refuse to sign on the previous page of this form, I know that this means I will not be able to receive assistance from the Program.
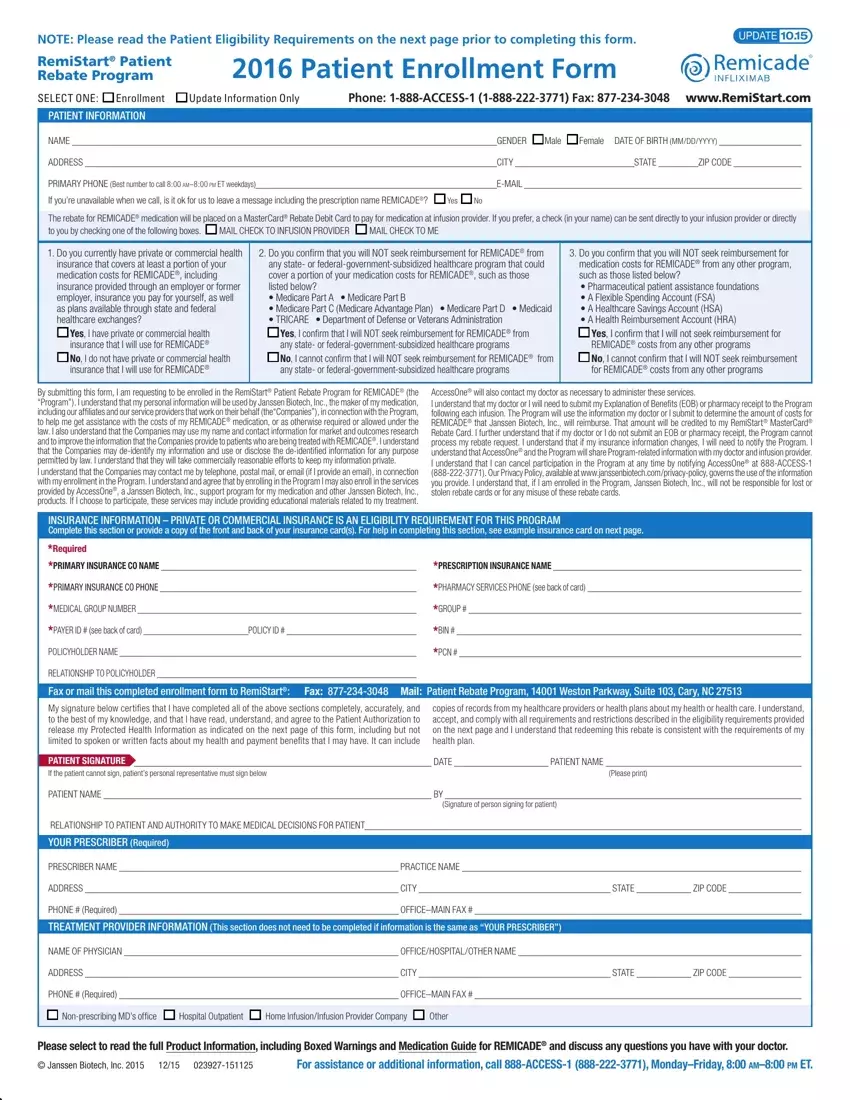
Patient Eligibility Requirements for the RemiStart® Program
RemiStart® is available to patients who:
•Are beginning or are currently receiving treatment with REMICADE®
•Currently have private or commercial health insurance that covers a portion of the medication costs for REMICADE®
Other Restrictions:
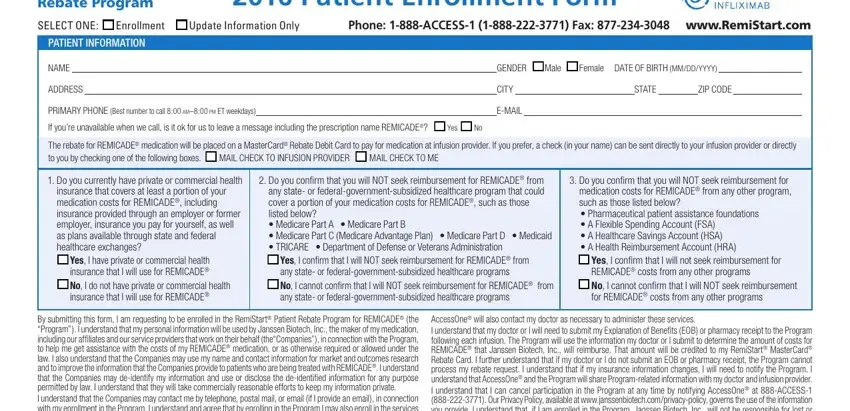
•This program is only available to individuals using private or commercial health insurance to cover a portion of their medication costs, including plans available through state and federal health care exchanges. This program is not available to individuals who use any state- or federal-government-subsidized healthcare program to cover a portion of medication costs, such as Medicare, Medicaid, TRICARE, Department of Defense, or Veterans Administration. Patients confirm that they will not seek reimbursement from any of these programs or from pharmaceutical patient assistance foundations and accounts such as a Flexible Spending Account (FSA), Healthcare Savings Account (HSA) or Health Reimbursement Account (HRA)
•This offer may not be combined with any other coupon, discount, prescription savings card, free trial, or other offer
•The selling, purchasing, trading, or counterfeiting of this rebate card is prohibited
•Offer good only in the U.S. and Puerto Rico. Janssen Biotech, Inc. reserves the right to rescind, revoke, or amend this offer without notice at any time. Void where prohibited, taxed, or otherwise restricted by law
•Offer for new enrollment expires December 31, 2016. For Massachusetts residents only, this offer is subject to change per state legislation
•This program is not retroactive
 MAIL CHECK TO INFUSION PROVIDER
MAIL CHECK TO INFUSION PROVIDER  MAIL CHECK TO ME
MAIL CHECK TO ME