
You could work with Renewal Form Husky effectively in our PDFinity® editor. We are dedicated to making sure you have the best possible experience with our tool by consistently adding new functions and improvements. Our tool is now a lot more user-friendly thanks to the latest updates! So now, working with documents is a lot easier and faster than before. If you're looking to start, here is what it will take:
Step 1: Access the PDF inside our editor by clicking the "Get Form Button" at the top of this page.
Step 2: The tool allows you to change nearly all PDF forms in a range of ways. Change it by writing any text, adjust original content, and place in a signature - all within the reach of a few clicks!
It's straightforward to complete the pdf following our helpful guide! This is what you have to do:
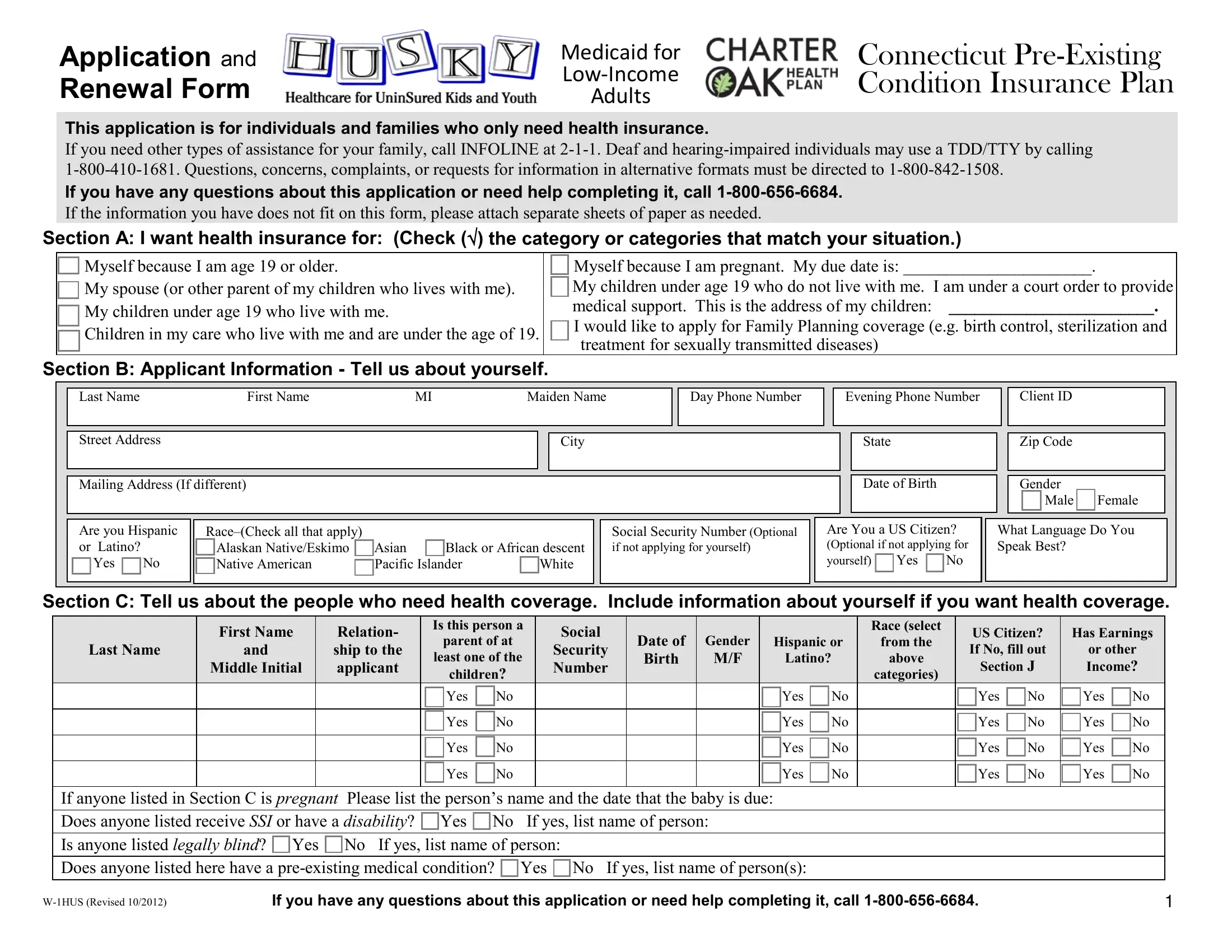
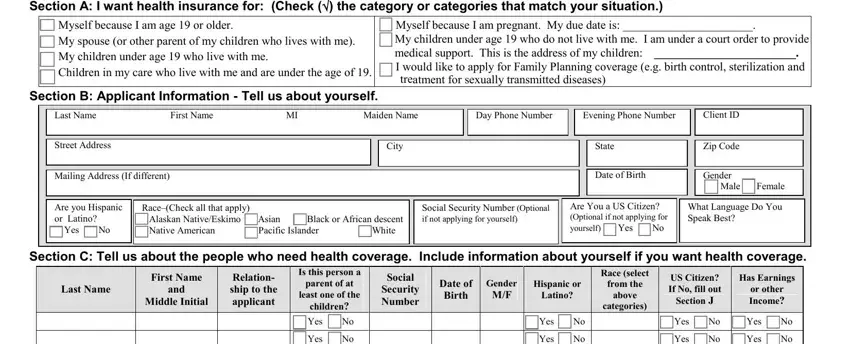
1. The Renewal Form Husky necessitates specific details to be typed in. Ensure the following fields are complete:
2. Now that this segment is finished, you'll want to put in the needed particulars in Middle Initial, If anyone listed in Section C is, Yes No Yes No Yes No Yes No, Yes No Yes No Yes No Yes No, Yes No Yes No Yes No Yes No, Yes No Yes No Yes No Yes No, WHUS Revised, and If you have any questions about allowing you to progress further.

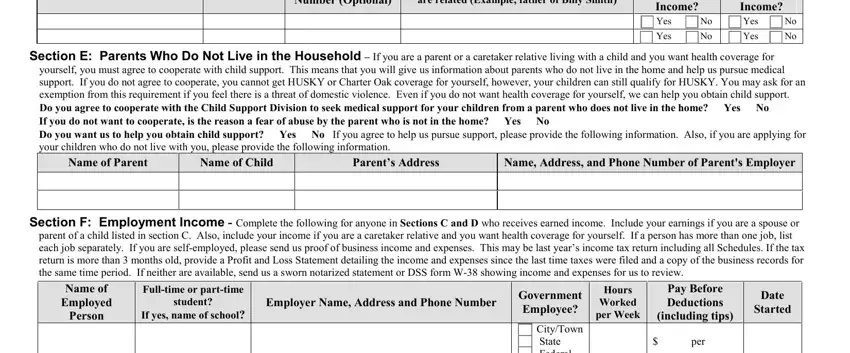
3. This 3rd part should be rather easy, Number Optional, are related Example father of, Receives Earned Income, Yes No Yes No, Income, Yes No Yes No, Section E Parents Who Do Not Live, yourself you must agree to, Name of Parent, Name of Child, Parents Address, Name Address and Phone Number of, Section F Employment Income, parent of a child listed in, and Employer Name Address and Phone - these form fields will have to be filled in here.
4. This next section requires some additional information. Ensure you complete all the necessary fields - Government Employee CityTown State, per, Section G Other Income Please, Name of Person, Type of Income, How Much, How Often, WHUS Revised, and If you have any questions about - to proceed further in your process!
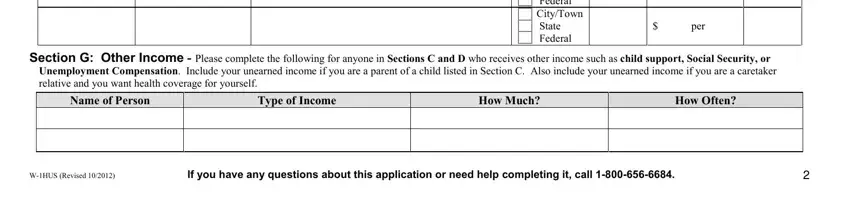
Lots of people frequently make errors when filling in Section G Other Income Please in this area. You need to go over whatever you enter right here.
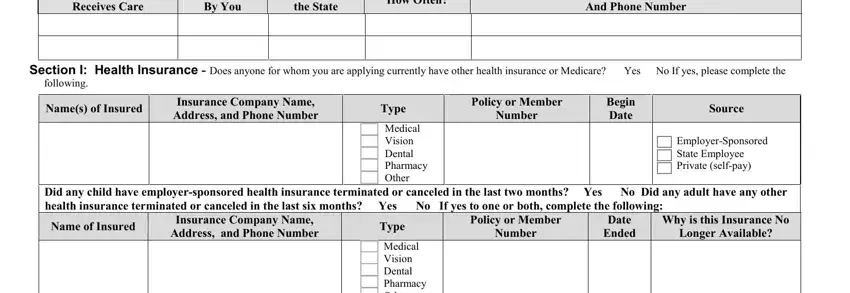
5. This form should be finalized by going through this section. Further there is a full set of form fields that require accurate details for your form usage to be complete: Receives Care, By You, the State, How Often, And Phone Number, Section I Health Insurance Does, following, Names of Insured, Insurance Company Name Address and, Type Medical Vision Dental, Policy or Member, Number, Begin Date, Source, and EmployerSponsored State Employee.
Step 3: Go through all the information you've typed into the form fields and then click the "Done" button. Make a free trial subscription with us and gain instant access to Renewal Form Husky - download or modify from your personal cabinet. When you use FormsPal, you can complete forms without needing to get worried about data leaks or entries being shared. Our protected platform ensures that your personal details are maintained safely.