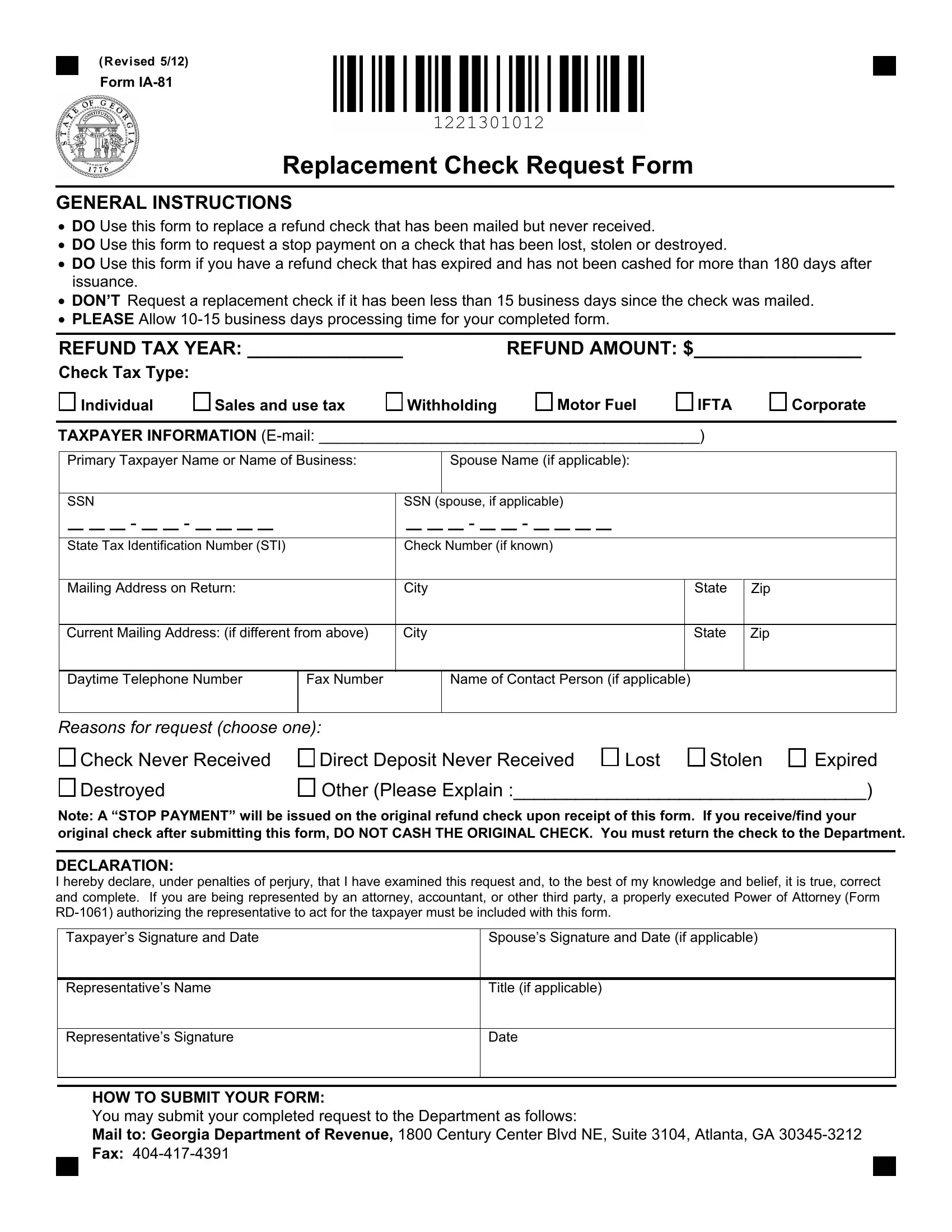
For individuals and businesses navigating the complexities of tax refund issues in Georgia, the Replacement Check Request Form, known as Form IA-81, serves as a crucial tool. Revised in May 2012, this form is specifically designed for instances where a refund check is either not received, lost, stolen, destroyed, or has expired without being cashed for more than 180 days after its issuance. It is important for taxpayers to understand the stipulations set forth by this form, such as the necessity to wait a minimum of 15 business days from the mailing date before submitting a request, and allowing for a processing time of 10-15 business days once the form has been completed and submitted. This form encompasses various tax types including individual, sales and use, withholding, motor fuel IFTA, and corporate taxes. Providing detailed taxpayer information, including the primary taxpayer or business name, social security numbers, state tax identification number, and both past and current mailing addresses, is imperative for the processing of the form. In addition, a concise declaration requirement emphasizes the need for accuracy and truthfulness under penalties of perjury. For taxpayers represented by a third party such as an attorney or accountant, a Power of Attorney (Form RD-1061) must also be included. Submission of the form can be done via mail or fax to the Georgia Department of Revenue, ensuring a methodical approach to resolving the issue of a misplaced or expired check, and reinstating the rightful funds to the taxpayer.
| Question | Answer |
|---|---|
| Form Name | Form IA-81 |
| Form Length | 1 pages |
| Fillable? | Yes |
| Fillable fields | 18 |
| Avg. time to fill out | 3 min 55 sec |
| Other names | E-mail, http dor georgia gov documents ia 81 replacement check request form, georgie state replacement check form taxes, check replacement form |
(Revised 5/12)
Form
Replacement Check Request Form
GENERAL INSTRUCTIONS
•DO Use this form to replace a refund check that has been mailed but never received.
•DO Use this form to request a stop payment on a check that has been lost, stolen or destroyed.
•DO Use this form if you have a refund check that has expired and has not been cashed for more than 180 days after issuance.
•DON’T Request a replacement check if it has been less than 15 business days since the check was mailed.
•PLEASE Allow
REFUND TAX YEAR: _____________ |
REFUND AMOUNT: $_______________ |
Check Tax Type:
Individual |
Sales and use tax |
Withholding |
Motor Fuel |
IFTA
Corporate
TAXPAYER INFORMATION
Primary Taxpayer Name or Name of Business: |
|
|
|
|
|
Spouse Name (if applicable): |
|
|
|
|||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
SSN |
|
|
|
|
|
|
|
|
|
|
SSN (spouse, if applicable) |
|
|
|
|
|
|
|
|
|||||||||||||||||||||||
|
|
|
|
|
|
- |
|
|
|
- |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
- |
|
|
|
- |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
State Tax Identification Number (STI) |
|
Check Number (if known) |
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Mailing Address on Return: |
|
City |
|
|
|
|
|
|
|
|
|
|
|
|
|
State |
Zip |
|
||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||
Current Mailing Address: (if different from above) |
City |
|
|
|
|
|
|
|
|
|
|
|
|
|
State |
Zip |
|
|||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
Daytime Telephone Number |
Fax Number |
|
|
|
|
|
Name of Contact Person (if applicable) |
|
|
|
||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Reasons for request (choose one): |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||
|
Check Never Received |
Direct Deposit Never Received |
|
|
|
Lost |
Stolen |
Expired |
||||||||||||||||||||||||||||||||||
|
Destroyed |
|
|
|
|
|
|
|
|
|
Other (Please Explain :__________________________________) |
|||||||||||||||||||||||||||||||
Note: A “STOP PAYMENT” will be issued on the original refund check upon receipt of this form. If you receive/find your original check after submitting this form, DO NOT CASH THE ORIGINAL CHECK. You must return the check to the Department.
DECLARATION:
I hereby declare, under penalties of perjury, that I have examined this request and, to the best of my knowledge and belief, it is true, correct and complete. If you are being represented by an attorney, accountant, or other third party, a properly executed Power of Attorney (Form
Taxpayer’s Signature and Date
Spouse’s Signature and Date (if applicable)
Representative’s Name
Title (if applicable)
Representative’s Signature
Date
HOW TO SUBMIT YOUR FORM:
You may submit your completed request to the Department as follows:
Mail to: Georgia Department of Revenue, 1800 Century Center Blvd NE, Suite 3104, Atlanta, GA
Fax: