
You'll be able to work with tx vaccine documentation form effectively by using our PDF editor online. To retain our editor on the leading edge of efficiency, we aim to adopt user-driven features and improvements regularly. We are always looking for suggestions - help us with remolding PDF editing. To get started on your journey, consider these basic steps:
Step 1: Click on the "Get Form" button above on this webpage to access our PDF editor.
Step 2: With our handy PDF tool, you can actually accomplish more than just complete blanks. Express yourself and make your forms appear high-quality with custom textual content added, or modify the file's original content to excellence - all comes along with the capability to add stunning images and sign the PDF off.
This PDF form needs specific details; to ensure accuracy and reliability, please make sure to bear in mind the guidelines further down:
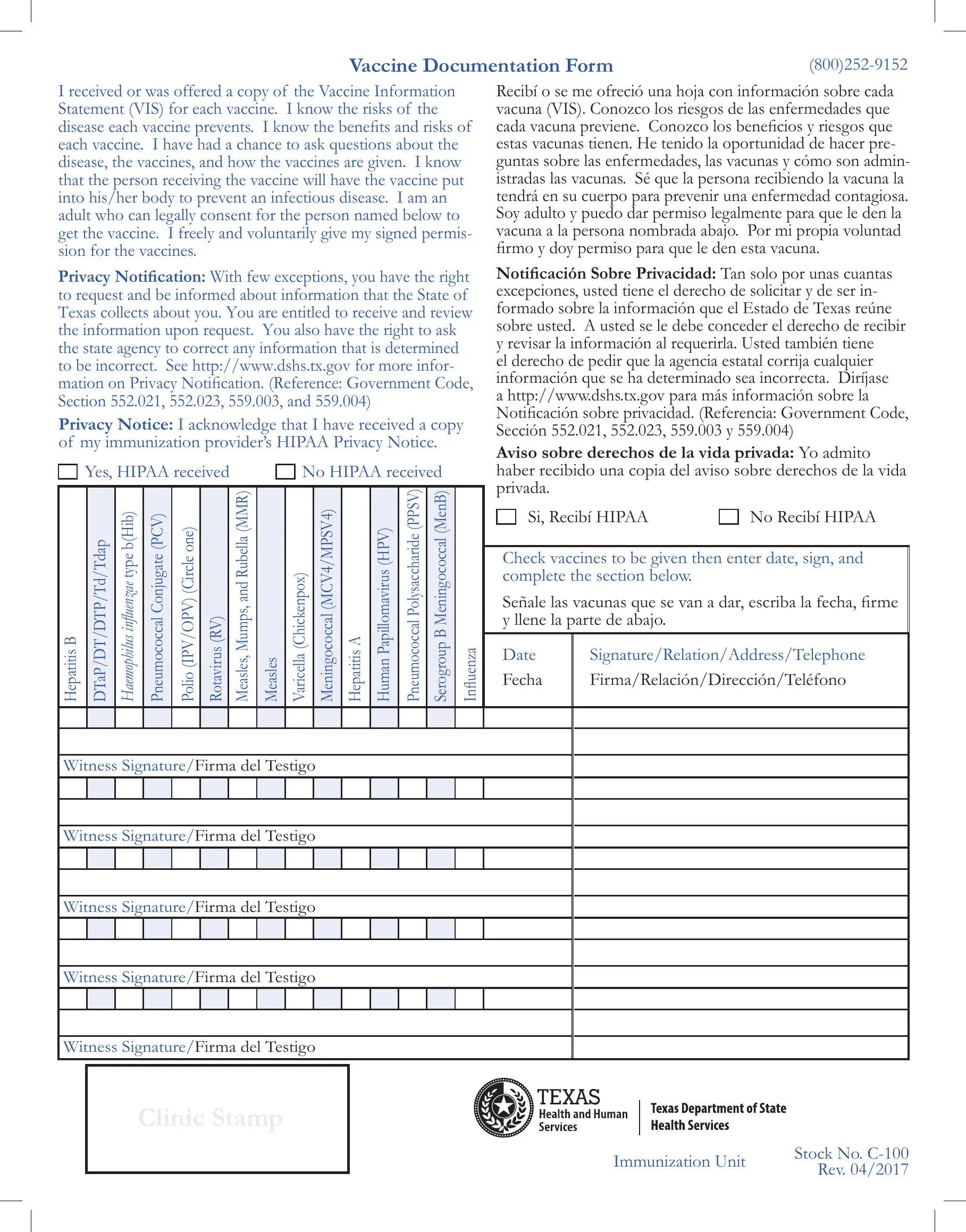
1. While filling out the tx vaccine documentation form, ensure to incorporate all essential blanks in its associated part. It will help facilitate the process, enabling your information to be processed promptly and properly.
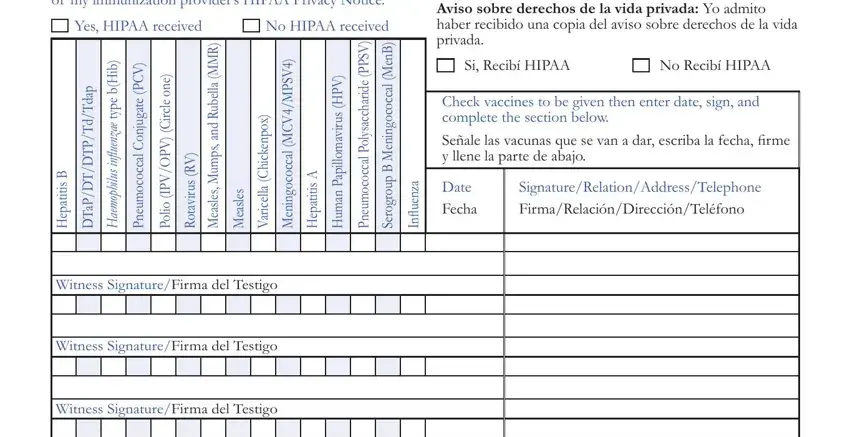
2. Right after the last section is filled out, go to type in the relevant details in all these - Witness SignatureFirma del Testigo, Witness SignatureFirma del Testigo, Clinic Stamp, Immunization Unit, and Stock No C Rev.
3. The following section is all about Date, Vaccine, Mfg, Lot No, Site Given, Given by, Date VIS Given, VIS Date, e n o, e l c r i, e n o e l c r i C, and Hepatitis B Hepatitis B Hepatitis - fill in all these blanks.
4. All set to complete this fourth segment! In this case you'll get all these Hepatitis B Hepatitis B Hepatitis, e l c r i C, and e n o fields to do.
It's easy to make errors when filling in your Hepatitis B Hepatitis B Hepatitis, thus be sure you reread it prior to when you finalize the form.
5. This final step to finish this form is pivotal. Be certain to fill out the appropriate blanks, for example LastApellido, FirstNombre, MiddleSegundo nombre Birth, AddressDirección, CityCiudad, Telephone NumberNúmero de, RaceRaza, StateEstado ZipCódigo postal, Social Security NumberNúmero de, Parents NameNombre del padre o de, and Mothers Maiden NameApellido de, before submitting. Or else, it might lead to an unfinished and probably unacceptable form!
Step 3: Make sure the information is correct and press "Done" to conclude the project. Right after registering a7-day free trial account at FormsPal, you will be able to download tx vaccine documentation form or send it via email directly. The PDF file will also be available via your personal account menu with your each and every change. We don't share or sell the information that you type in whenever working with forms at our site.