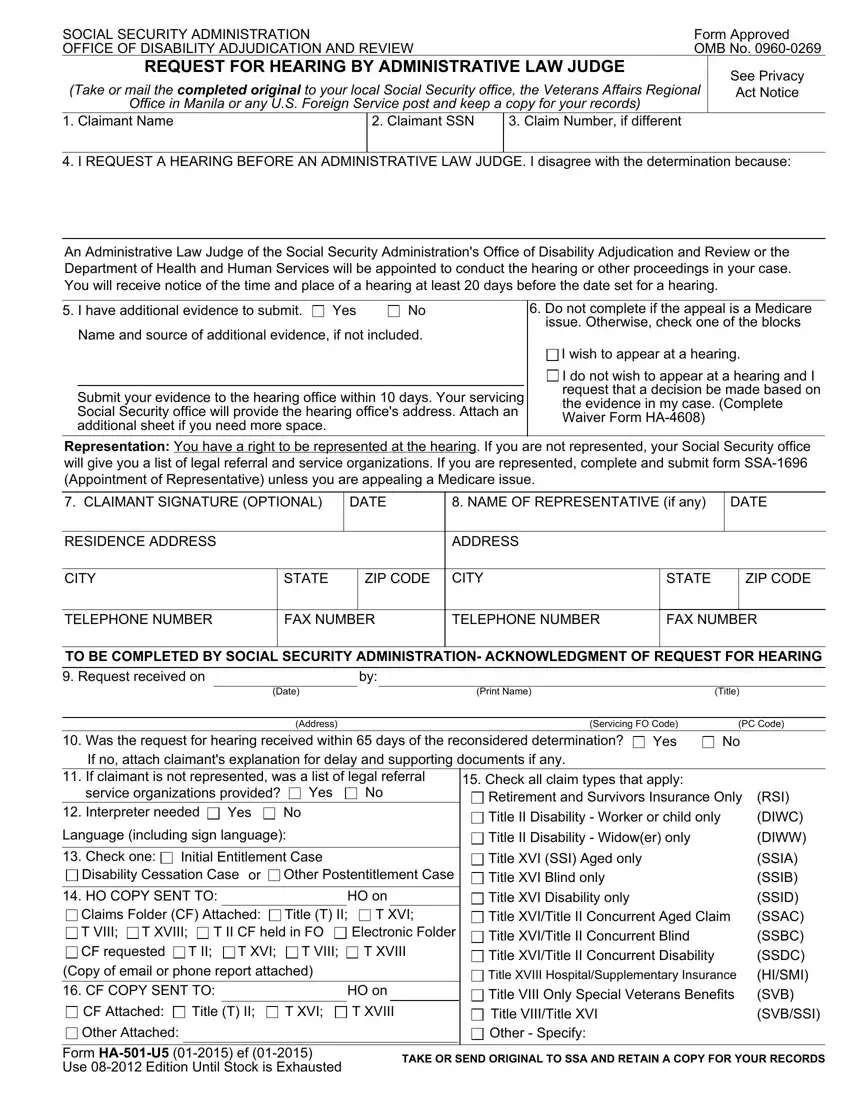

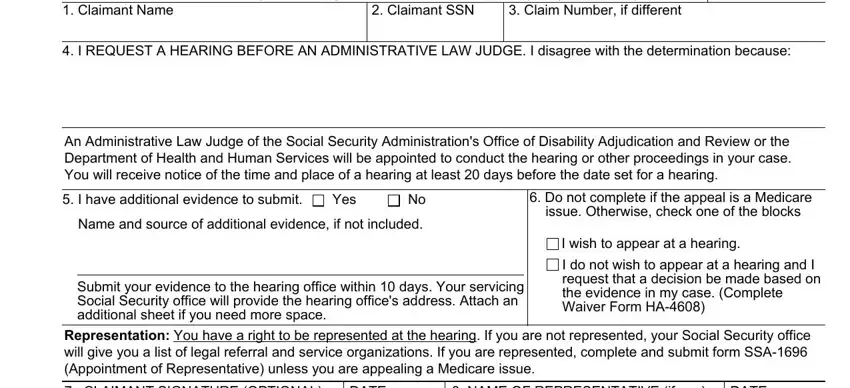
 I wish to appear at a hearing.
I wish to appear at a hearing. I do not wish to appear at a hearing and I request that a decision be made based on the evidence in my case. (Complete Waiver Form
I do not wish to appear at a hearing and I request that a decision be made based on the evidence in my case. (Complete Waiver Form 
It's simple to complete the ssa 501 gaps. Our PDF editor makes it nearly effortless to complete any specific PDF file. Below are the basic four steps you should take:
Step 1: You should click the orange "Get Form Now" button at the top of the webpage.
Step 2: After you have accessed your ssa 501 edit page, you'll see all functions you can take with regards to your file within the upper menu.
The PDF file you wish to fill out will include the following parts:
You need to fill out the CLAIMANT SIGNATURE OPTIONAL, DATE, NAME OF REPRESENTATIVE if any, DATE, RESIDENCE ADDRESS, ADDRESS, CITY, STATE, ZIP CODE, CITY, STATE, ZIP CODE, TELEPHONE NUMBER, FAX NUMBER, and TELEPHONE NUMBER box with the required data.
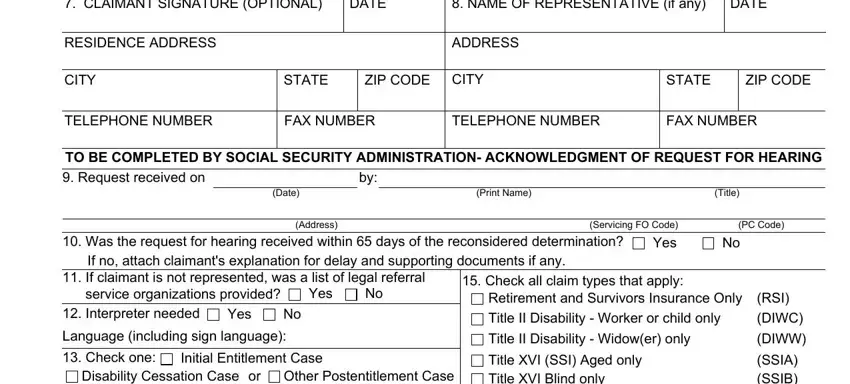
Determine the relevant data in the Disability Cessation Case, Other Postentitlement Case, Initial Entitlement Case or, HO COPY SENT TO, HO on, Claims Folder CF Attached T VIII T, T II, T XVI, Title T II, T XVI, T II CF held in FO, Electronic Folder, T VIII, T XVIII, and Copy of email or phone report box.
The PRIVACY ACT STATEMENT Request for, Sections a USC a USC e A and, Providing this information is, We rarely use the information you, To enable a third party or an, Security benefits andor coverage, To comply with Federal laws, eg to the Government, To make determinations for, Federal State and local level and, and To facilitate statistical section is the place where each side can insert their rights and responsibilities.
Finish the file by checking these particular fields: A complete list of routine uses, This information collection meets, wwwsocialsecuritygov, and Form HAU ef.
Step 3: Press the "Done" button. Then, you can transfer your PDF document - upload it to your device or deliver it via email.
Step 4: It may be more convenient to create duplicates of your form. There is no doubt that we will not reveal or view your particulars.
