
dhs rule 25 can be filled in online very easily. Just use FormsPal PDF editing tool to finish the job promptly. FormsPal expert team is ceaselessly working to develop the tool and make it even easier for people with its multiple functions. Discover an ceaselessly revolutionary experience today - explore and find out new possibilities along the way! To begin your journey, take these easy steps:
Step 1: Click on the "Get Form" button at the top of this page to open our PDF editor.
Step 2: This tool helps you change your PDF form in a variety of ways. Modify it with personalized text, correct original content, and include a signature - all within a few mouse clicks!
As a way to finalize this PDF form, be sure you type in the right information in each and every field:
1. To start off, when filling out the dhs rule 25, start in the section that contains the subsequent blanks:
2. Now that the previous section is completed, you'll want to include the needed particulars in This interview was not completed, Reason, Actions taken, PMI or insurance number, and DHS Rule Assessment of so you're able to move forward to the next part.
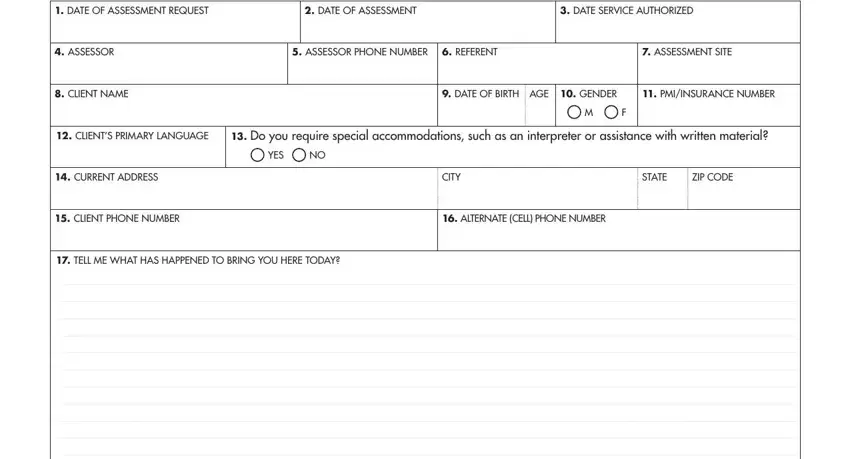
3. Through this step, examine DATE OF ASSESSMENT REQUEST, DATE OF ASSESSMENT, DATE SERVICE AUTHORIZED, ASSESSOR, ASSESSOR PHONE NUMBER, REFERENT, ASSESSMENT SITE, CLIENT NAME, DATE OF BIRTH AGE GENDER, PMIINSURANCE NUMBER, CLIENTS PRIMARY LANGUAGE, Do you require special, YES, CURRENT ADDRESS, and CITY. Each one of these should be filled out with greatest accuracy.
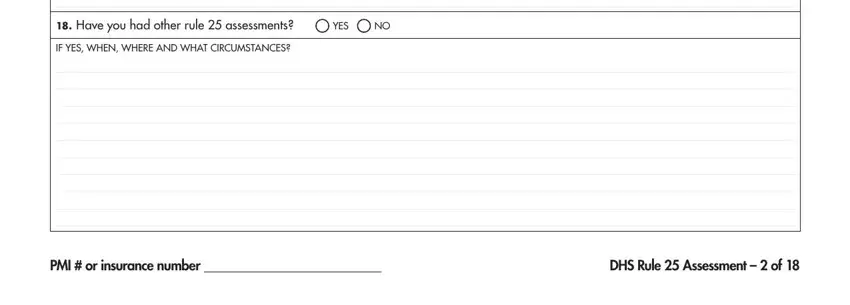
4. The fourth paragraph comes next with these particular fields to focus on: Have you had other rule, YES, IF YES WHEN WHERE AND WHAT, PMI or insurance number, and DHS Rule Assessment of.
5. Because you come close to the end of the file, you'll notice a few more points to complete. Specifically, Age of First Use, Need enough information to show, if needed, Withdrawal Potential, Method of use oral smoked snort, Needs special care DSM, IV etc, X Primary Drug Used, ALCOHOL, MARIJUANAHASHISH, COCAINECRACK, METHAMPHETAMINES, HEROIN, OTHER OPIATES, and SYNTHETICS should be done.
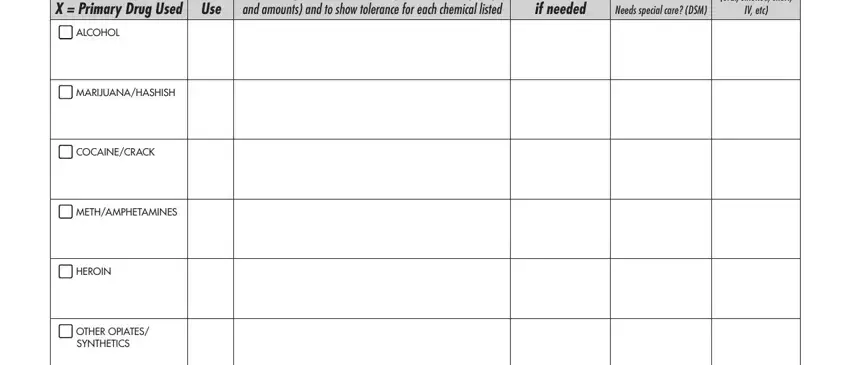
Be very attentive when filling in X Primary Drug Used and SYNTHETICS, since this is where many people make mistakes.
Step 3: Before finalizing the document, double-check that all form fields have been filled out the proper way. The moment you verify that it's fine, click on “Done." Make a 7-day free trial subscription with us and obtain instant access to dhs rule 25 - download or modify inside your FormsPal cabinet. FormsPal ensures your data privacy by having a protected system that in no way saves or distributes any kind of private data used in the form. You can relax knowing your documents are kept protected any time you use our editor!