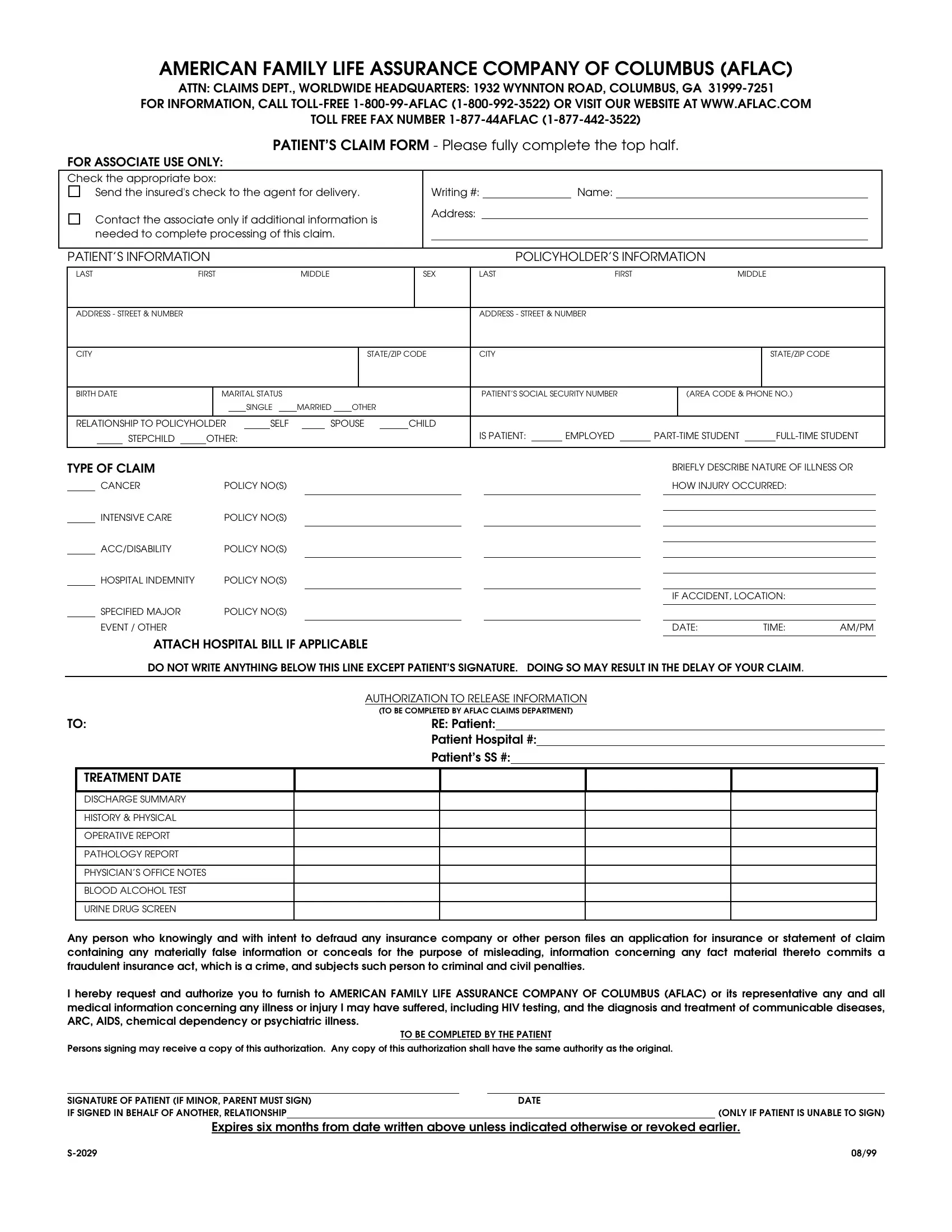
In an era where precise documentation is key to ensuring smooth insurance claim processes, understanding the intricacies of forms like the S 2029 becomes indispensable. Crafted for policyholders under the American Family Life Assurance Company of Columbus, commonly known as AFLAC, this form is designed to facilitate the submission of claims, whether they relate to accidents, disabilities, intensive care, or cancer policies among others. It serves as a vital communication tool between the claimant and AFLAC, necessitating detailed completion for a hassle-free claim experience. The form is segmented into various sections, each requiring specific information about the patient, the policyholder, and the nature of the claim itself, accompanied by a physician's statement for a comprehensive understanding of the medical scenario. At the heart of it, the S 2029 form emphasizes transparency and accuracy in reporting the claim details, underlined by the stern warning against fraudulent claims. Moreover, the form underscores the importance of consent, with a section dedicated to authorizing AFLAC or its representatives access to essential medical records, thereby balancing the need for information with the privacy rights of the individual. This delicate interplay of providing accurate, detailed information while adhering to legal and ethical standards defines the essence of the S 2029 form and its role in the broader context of insurance claims.
| Question | Answer |
|---|---|
| Form Name | S 2029 Form |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | aflac cancer claim forms to print, aflac cancer claim forms print, aflac claim forms cancer continuing to print, skin cancer aflac claim forms print |
AMERICAN FAMILY LIFE ASSURANCE COMPANY OF COLUMBUS (AFLAC)
ATTN: CLAIMS DEPT., WORLDWIDE HEADQUARTERS: 1932 WYNNTON ROAD, COLUMBUS, GA
FOR INFORMATION, CALL
TOLL FREE FAX NUMBER
PATIENT’S CLAIM FORM - Please fully complete the top half.
FOR ASSOCIATE USE ONLY:
Check the appropriate box:
Send the insured's check to the agent for delivery.
Contact the associate only if additional information is needed to complete processing of this claim.
Writing #: |
|
Name: |
Address:
PATIENT’S INFORMATION |
|
|
|
|
|
|
|
|
|
|
|
|
|
POLICYHOLDER’S INFORMATION |
|
|
|||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
LAST |
FIRST |
|
|
|
MIDDLE |
|
|
|
SEX |
LAST |
|
FIRST |
|
MIDDLE |
|
|
|||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
ADDRESS - STREET & NUMBER |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
ADDRESS - STREET & NUMBER |
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
CITY |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
STATE/ZIP CODE |
CITY |
|
|
|
|
|
|
|
STATE/ZIP CODE |
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
BIRTH DATE |
|
|
MARITAL STATUS |
|
|
|
|
|
|
|
|
|
|
PATIENT’S SOCIAL SECURITY NUMBER |
|
(AREA CODE & PHONE NO.) |
|||||||||||||||
|
|
|
|
|
|
|
|
|
SINGLE |
|
MARRIED OTHER |
|
|
|
|
|
|
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
RELATIONSHIP TO POLICYHOLDER |
|
|
SELF |
|
|
SPOUSE |
|
|
CHILD |
|
|
|
|
|
|
|
|
|
|
||||||||||||
|
|
STEPCHILD |
|
OTHER: |
|
|
|
|
|
|
|
|
|
|
|
|
|
IS PATIENT: |
|
EMPLOYED |
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
TYPE OF CLAIM
CANCER |
POLICY NO(S) |
INTENSIVE CARE |
POLICY NO(S) |
ACC/DISABILITY |
POLICY NO(S) |
HOSPITAL INDEMNITY |
POLICY NO(S) |
BRIEFLY DESCRIBE NATURE OF ILLNESS OR HOW INJURY OCCURRED:
IF ACCIDENT, LOCATION:
|
|
|
SPECIFIED MAJOR |
POLICY NO(S) |
|
|
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
EVENT / OTHER |
|
|
|
|
|
|
|
|
|
|
|
DATE: |
TIME: |
AM/PM |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
ATTACH HOSPITAL BILL IF APPLICABLE |
|
|
|
|
||||||||||||
|
|
|
DO NOT WRITE ANYTHING BELOW THIS LINE EXCEPT PATIENT’S SIGNATURE. DOING SO MAY RESULT IN THE DELAY OF YOUR CLAIM. |
|
|
|
|||||||||||||
|
|
|
|
|
|
AUTHORIZATION TO RELEASE INFORMATION |
|
|
|
|
|||||||||
|
|
|
|
|
|
(TO BE COMPLETED BY AFLAC CLAIMS DEPARTMENT) |
|
|
|
|
|||||||||
TO: |
|
|
RE: Patient: |
|
|
|
|
|
|||||||||||
|
|
|
|
|
|
Patient Hospital #: |
|
|
|
|
|||||||||
|
|
|
|
|
|
Patient’s SS #: |
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
TREATMENT DATE |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
DISCHARGE SUMMARY |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
HISTORY & PHYSICAL |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
OPERATIVE REPORT |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
PATHOLOGY REPORT |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
PHYSICIAN’S OFFICE NOTES |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
BLOOD ALCOHOL TEST |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
URINE DRUG SCREEN |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Any person who knowingly and with intent to defraud any insurance company or other person files an application for insurance or statement of claim containing any materially false information or conceals for the purpose of misleading, information concerning any fact material thereto commits a fraudulent insurance act, which is a crime, and subjects such person to criminal and civil penalties.
I hereby request and authorize you to furnish to AMERICAN FAMILY LIFE ASSURANCE COMPANY OF COLUMBUS (AFLAC) or its representative any and all medical information concerning any illness or injury I may have suffered, including HIV testing, and the diagnosis and treatment of communicable diseases, ARC, AIDS, chemical dependency or psychiatric illness.
|
|
TO BE COMPLETED BY THE PATIENT |
|||
Persons signing may receive a copy of this authorization. Any copy of this authorization shall have the same authority as the original. |
|||||
|
|
|
|
|
|
SIGNATURE OF PATIENT (IF MINOR, PARENT MUST SIGN) |
|
|
DATE |
||
IF SIGNED IN BEHALF OF ANOTHER, RELATIONSHIP |
|
|
|
|
(ONLY IF PATIENT IS UNABLE TO SIGN) |
Expires six months from date written above unless indicated otherwise or revoked earlier.
08/99 |
PHYSICIAN’S STATEMENT
AMERICAN FAMILY LIFE ASSURANCE COMPANY OF COLUMBUS (AFLAC)
ATTN: CLAIMS DEPT., WORLDWIDE HEADQUARTERS: 1932 WYNNTON ROAD, COLUMBUS, GA
|
|
|
|
|
|
|
|
TO BE COMPLETED IN FULL BY ATTENDING PHYSICIAN |
|
|
|
|
|
|
|
|||||||||
PATIENT’S INFORMATION |
|
|
|
|
|
|
|
|
|
|
POLICYHOLDER’S INFORMATION |
|
||||||||||||
LAST |
FIRST |
MIDDLE |
|
|
SEX |
LAST |
|
|
|
|
FIRST |
|
|
|
MIDDLE |
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
ADDRESS - STREET & NUMBER |
|
|
|
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
CITY |
|
|
|
|
|
|
|
STATE/ZIP CODE |
|
CITY |
|
|
|
|
|
|
|
|
|
STATE/ZIP CODE |
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
BIRTH DATE |
|
STATUS |
|
|
|
|
|
|
|
PATIENT’S RELATIONSHIP TO POLICYHOLDER: |
|
|
PHONE |
|||||||||||
|
|
|
SINGLE |
MARRIED |
OTHER: |
|
|
SELF |
|
SPOUSE |
CHILD |
|
STEPCHILD |
|
OTHER: |
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
POLICY NUMBER(S):
Any person who knowingly and with intent to defraud any insurance company or other person files an application for insurance or statement of claim containing any materially false information or conceals for the purpose of misleading, information concerning any fact material thereto commits a fraudulent insurance act, which is a crime, and subjects such person to criminal and civil penalties.
DIAGNOSIS |
|
|
|
|
IF INJURY, GIVE DATE AND PLACE OF INCIDENT. |
|
1. |
|
ICD |
|
|
|
|
2. |
|
ICD |
|
|
IF LOSS IS DUE TO ACCIDENTAL INJURY, EXPLAIN HOW ACCIDENT OCCURRED. |
|
LIST ANY CHRONIC ILLNESS OR DISEASE |
|
|
|
|
|
|
1. |
|
ONSET DATE |
|
|
|
|
2. |
|
ONSET DATE |
|
|
|
|
3. |
|
ONSET DATE |
|
|
|
|
IF AUTO ACCIDENT, WAS PATIENT
DRIVER PASSENGER UNKNOWN
IS THIS ACCIDENT/ILLNESS COVERED BY WORKER’S COMPENSATION?
YESNO
IS THIS ACCIDENT/ILLNESS COVERED BY MEDICAID / STATE AID?
YESNO
1. |
DATE SYMPTOMS FIRST OCCURRED |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
DATE PATIENT FIRST CONSULTED YOU FOR THIS CONDITION |
|
|
|
||||||||||||||||
2. |
HAS PATIENT EVER HAD SAME OR SIMILAR CONDITION? |
|
|
NO |
|
|
YES (IF YES, STATE WHEN AND DESCRIBE) |
|
|
|
|
|
|
|
|||||||||||||||||||||||
3. |
REFERRING PHYSICIAN (NAME/ADDRESS |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
4. |
WAS PATIENT HOSPITALIZED FOR THIS CONDITION? |
|
|
|
|
NO |
|
YES IF YES, HAVE CLAIMANT ATTACH A COPY OF THE ITEMIZED HOSPITAL BILLING WHEN SUBMITTING CLAIM FOR |
|||||||||||||||||||||||||||||
|
REVIEW . |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
5. |
DATE PATIENT LAST EXAMINED BY YOU |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
FREQUENCY OF VISITS |
|
WEEKLY |
|
|
|
MONTHLY |
|
OTHER |
|||||||||||
6. |
IS PATIENT UNABLE TO PERFORM JOB DUTIES? |
|
|
NO |
|
|
|
|
|
|
YES (IF YES, GIVE DATES) |
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||
7. |
WHAT SPECIFIC JOB DUTIES IS PATIENT UNABLE TO PERFORM? |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||
8. |
IS PATIENT |
|
AMBULATORY |
|
BED CONFINED |
|
|
|
|
HOUSE CONFINED |
|
|
HOSPITAL CONFINED |
|
|
OTHER |
|
|
|
||||||||||||||||||
9. |
IF RETIRED, WHICH ACTIVITIES OF DAILY LIVING (ADLs) IS PATIENT UNABLE TO PERFORM? |
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||
DATES OF SERVICE
PLACE OF
SERVICE
IN/OP
PROCEDURE DESCRIPTION
# UNITS
CODE
CPT
HCPCS/RVS
DIAGNOSIS CODE ICD.0
CHARGE
Date |
|
SIGNED |
Name of Attending Physician (Please Print)
Tax ID or Social Security Number
(Street Address) |
(City or Town) |
(State) |
(Zip Code) |
(Area Code - Phone) |
I hereby request and authorize you to furnish to AMERICAN FAMILY LIFE ASSURANCE COMPANY OF COLUMBUS (AFLAC) or its representative any and all medical information concerning any illness or injury I may have suffered including HIV testing and the diagnosis and treatment of communicable diseases, ARC, AIDS, chemical dependency or psychiatric illness.
Persons signing may receive a copy of this authorization. Any copy of this authorization shall have the same authority as the original.
SIGNATURE OF PATIENT (IF MINOR, PARENT MUST SIGN) |
DATE |
||
|
|
( Expires six months from this date unless indicated or revoked earlier.) |
|
If signed on behalf of another, relationship |
|
|
(Only if patient is unable to sign) |
08/99 |