
saif 801 form pdf can be filled in with ease. Simply try FormsPal PDF editing tool to accomplish the job right away. To make our tool better and easier to use, we constantly implement new features, with our users' feedback in mind. This is what you'll want to do to get started:
Step 1: Simply click on the "Get Form Button" in the top section of this site to see our pdf file editor. There you'll find everything that is required to fill out your file.
Step 2: After you access the PDF editor, you will get the form ready to be completed. Besides filling out various blank fields, it's also possible to do several other actions with the PDF, such as writing any textual content, modifying the initial text, adding illustrations or photos, putting your signature on the PDF, and a lot more.
It really is straightforward to complete the document with our detailed guide! Here's what you should do:
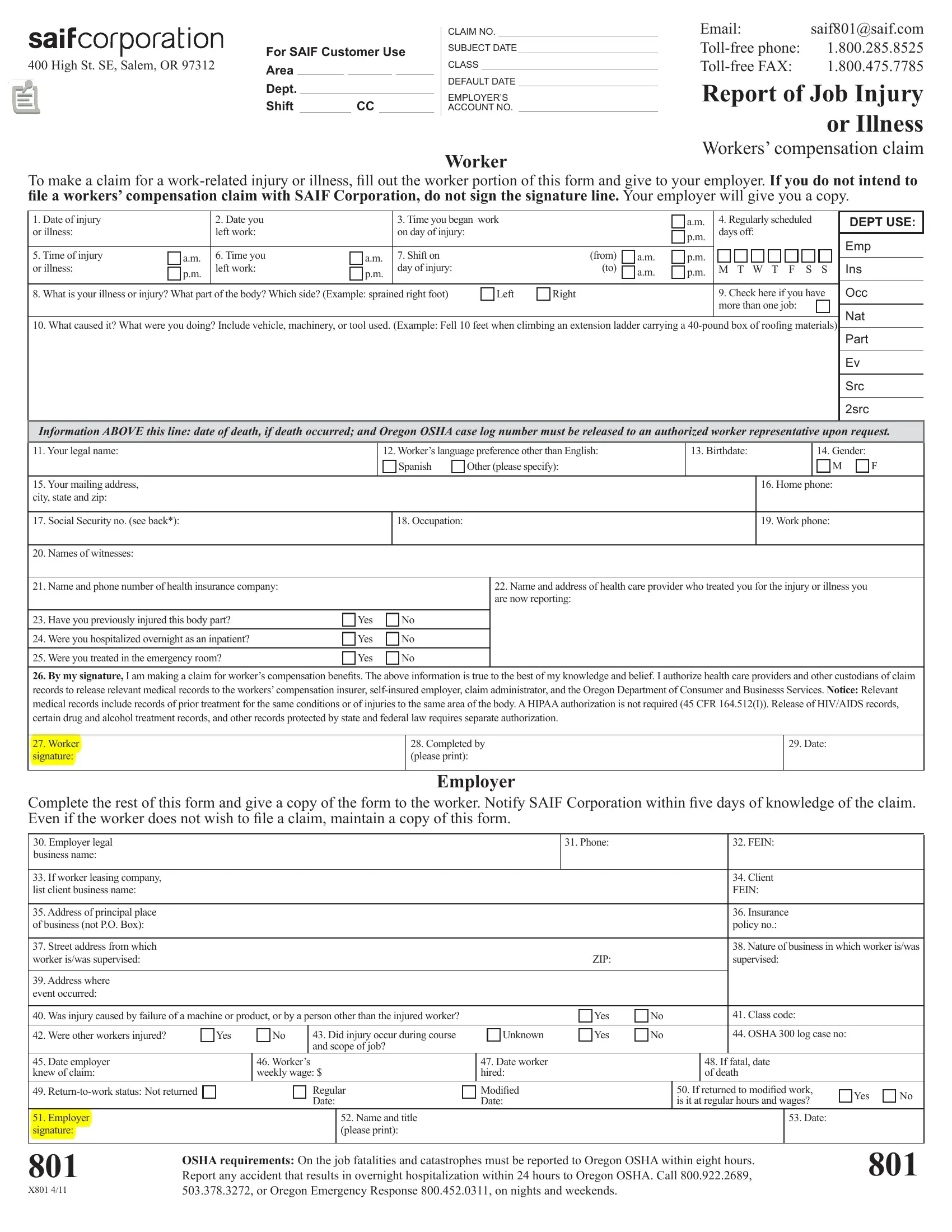
1. Fill out the saif 801 form pdf with a selection of major blank fields. Get all of the necessary information and be sure not a single thing overlooked!
2. The third step would be to fill out all of the following blank fields: Names of witnesses, Name and phone number of health, Name and address of health care, Have you previously injured this, Yes Yes Yes, No No No, Worker signature, Completed by please print, Date, Complete the rest of this form and, Phone, FEIN, Employer, If worker leasing company list, and Address of principal place of.
Concerning If worker leasing company list and Completed by please print, be sure you get them right here. The two of these could be the most significant ones in the file.
3. In this stage, examine Address where event occurred, Was injury caused by failure of a, Yes, Date employer knew of claim, Employer signature, Workers weekly wage, Regular Date, Name and title please print, Unknown, Date worker hired Modiied Date, Yes Yes, No No, Class code OSHA log case no, If fatal date of death, and If returned to modiied work is it. These will have to be completed with greatest precision.
Step 3: Immediately after going through the fields you've filled out, hit "Done" and you are done and dusted! Right after registering a7-day free trial account at FormsPal, you'll be able to download saif 801 form pdf or email it at once. The form will also be at your disposal via your personal cabinet with your each change. When using FormsPal, you'll be able to fill out documents without stressing about information leaks or entries getting distributed. Our secure system makes sure that your personal information is kept safely.