Our top rated developers have worked collectively to make the PDF editor that you could benefit from. The following application makes it simple to get medical certificate sc ins5140 forms instantly and effortlessly. This is all you have to carry out.
Step 1: Press the "Get Form Now" button to get started on.
Step 2: The document editing page is now open. You can include text or modify existing information.
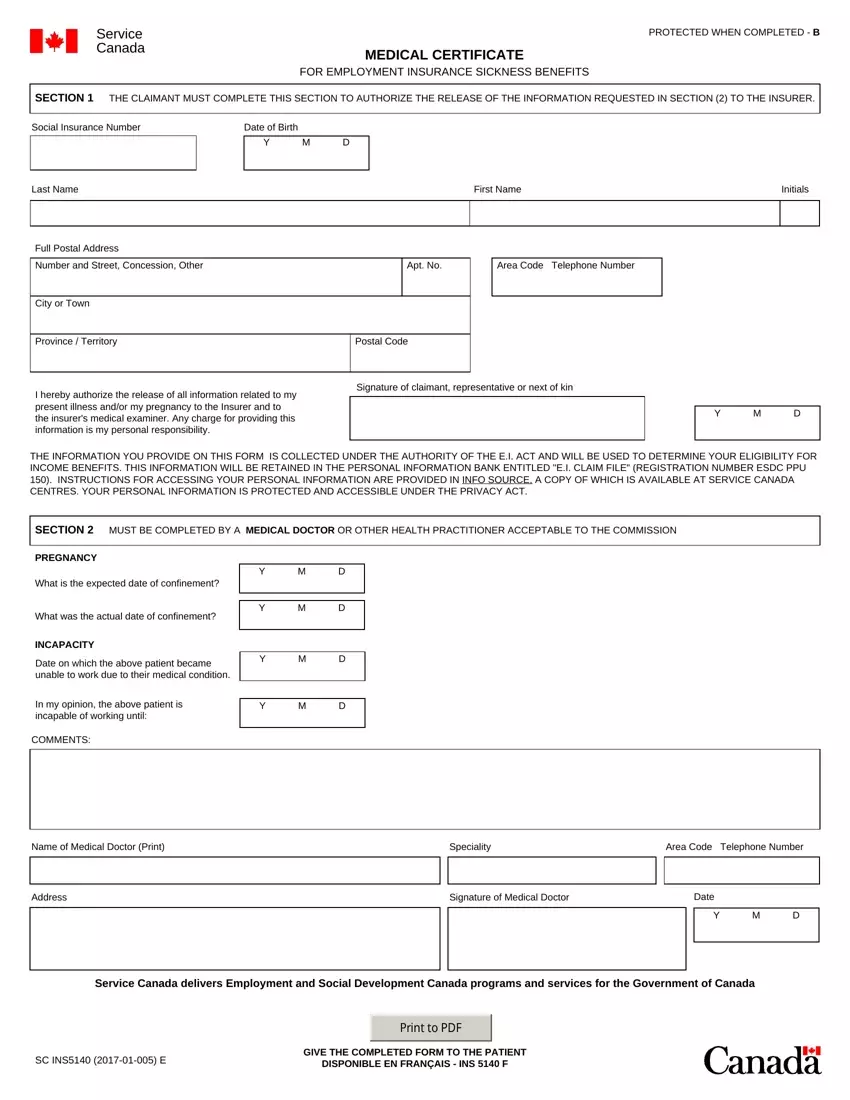
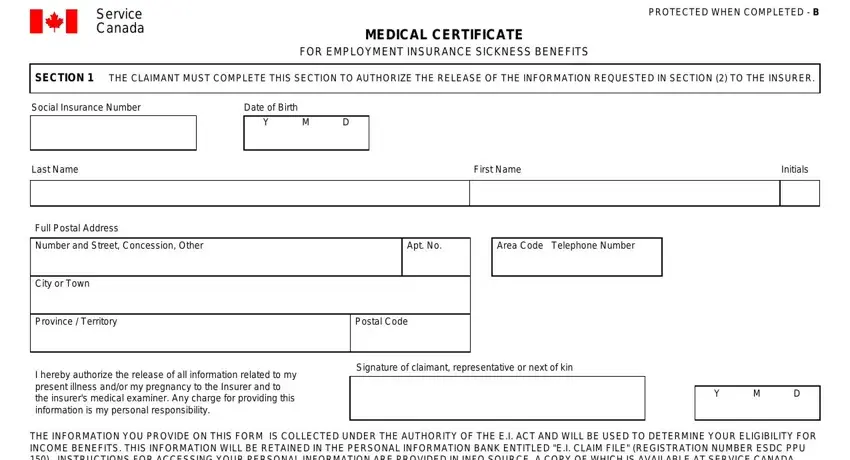
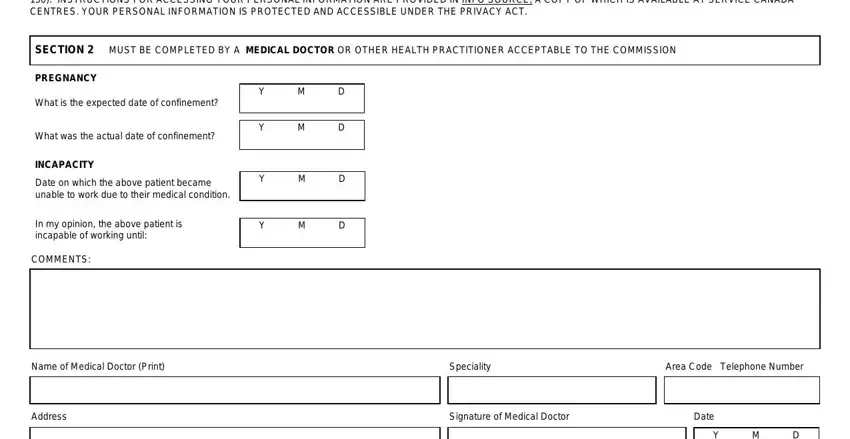
Prepare the medical certificate sc ins5140 PDF by providing the data needed for each individual part.
Write the information in .
The system will request you to provide certain fundamental details to easily complete the part .
Step 3: When you select the Done button, your ready form can be simply transferred to any kind of your gadgets or to electronic mail provided by you.
Step 4: It may be better to prepare copies of the document. You can rest assured that we won't display or check out your information.
