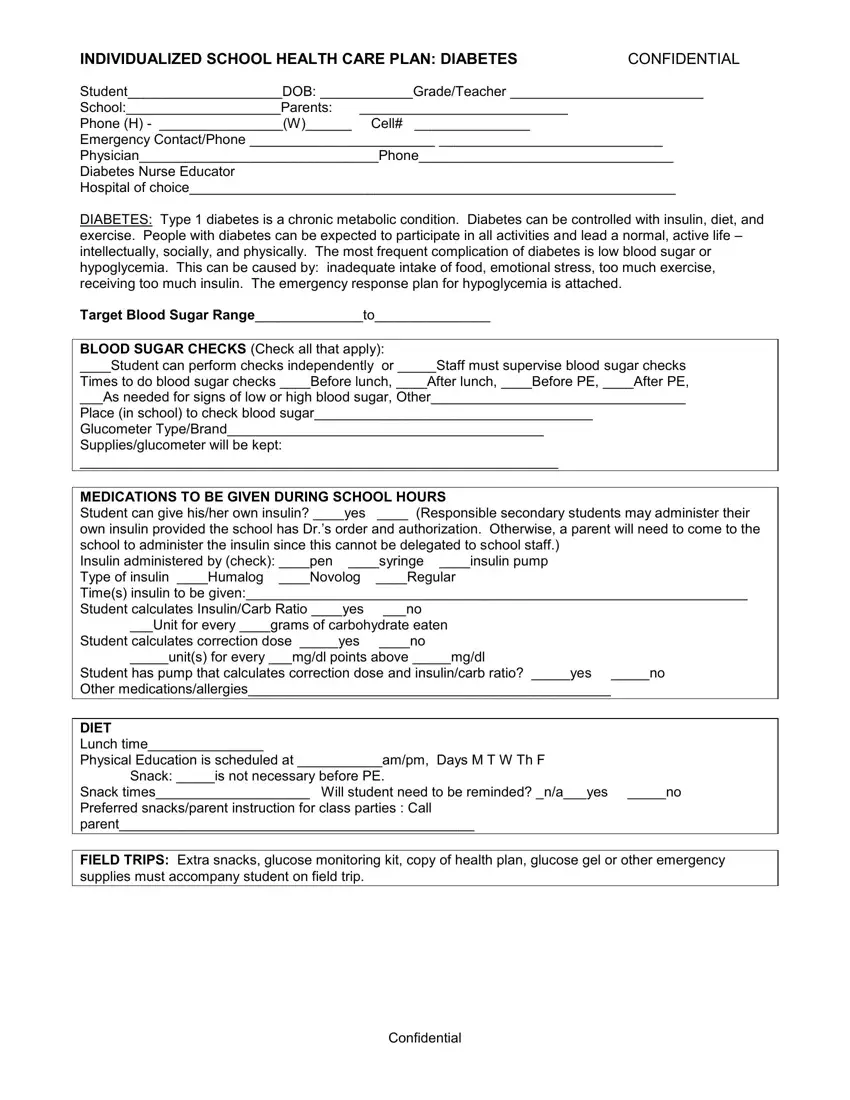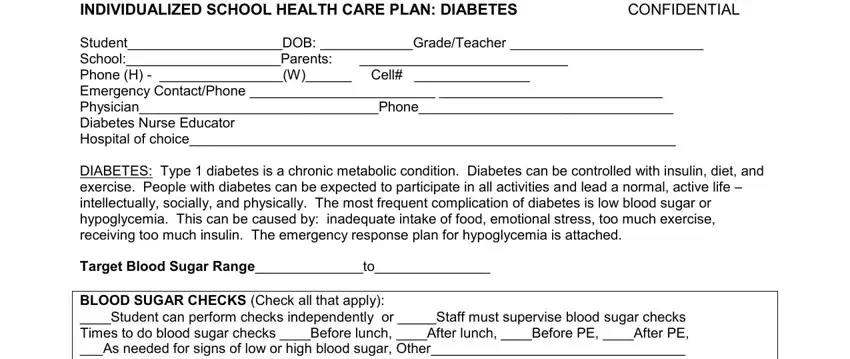
INDIVIDUALIZED SCHOOL HEALTH CARE PLAN: DIABETES |
CONFIDENTIAL |
Student____________________DOB: ____________Grade/Teacher _________________________ |
School:____________________Parents: |
___________________________ |
|
Phone (H) - ________________(W)______ |
Cell# _______________ |
|
Emergency Contact/Phone ________________________ _____________________________
Physician_______________________________Phone_________________________________
Diabetes Nurse Educator
Hospital of choice_______________________________________________________________
DIABETES: Type 1 diabetes is a chronic metabolic condition. Diabetes can be controlled with insulin, diet, and exercise. People with diabetes can be expected to participate in all activities and lead a normal, active life – intellectually, socially, and physically. The most frequent complication of diabetes is low blood sugar or hypoglycemia. This can be caused by: inadequate intake of food, emotional stress, too much exercise, receiving too much insulin. The emergency response plan for hypoglycemia is attached.
Target Blood Sugar Range______________to_______________
BLOOD SUGAR CHECKS (Check all that apply):
____Student can perform checks independently or _____Staff must supervise blood sugar checks
Times to do blood sugar checks ____Before lunch, ____After lunch, ____Before PE, ____After PE,
___As needed for signs of low or high blood sugar, Other_________________________________
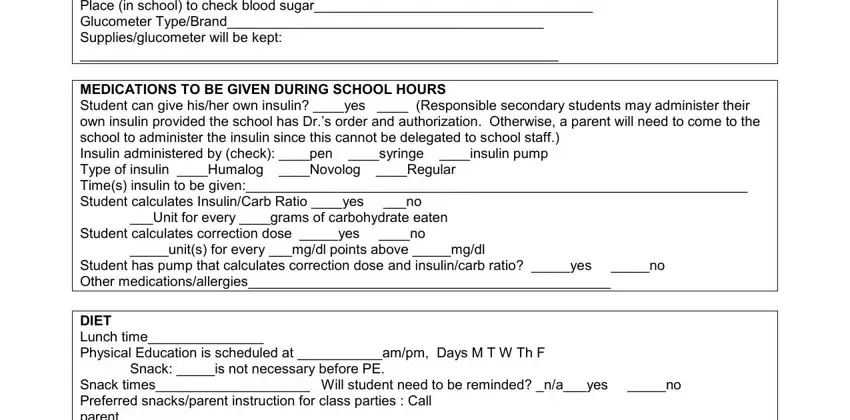
Place (in school) to check blood sugar____________________________________
Glucometer Type/Brand_________________________________________
Supplies/glucometer will be kept:
______________________________________________________________
MEDICATIONS TO BE GIVEN DURING SCHOOL HOURS
Student can give his/her own insulin? ____yes ____ (Responsible secondary students may administer their
own insulin provided the school has Dr.’s order and authorization. Otherwise, a parent will need to come to the school to administer the insulin since this cannot be delegated to school staff.)
Insulin administered by (check): ____pen ____syringe ____insulin pump
Type of insulin ____Humalog ____Novolog ____Regular
Time(s) insulin to be given:_________________________________________________________________
Student calculates Insulin/Carb Ratio ____yes |
___no |
|
___Unit for every ____grams of carbohydrate eaten |
|
Student calculates correction dose _____yes |
____no |
|
_____unit(s) for every ___mg/dl points above _____mg/dl |
|
Student has pump that calculates correction dose and insulin/carb ratio? _____yes |
_____no |
Other medications/allergies_______________________________________________ |
|
|
|
|
DIET |
|
|
Lunch time_______________ |
|
|
Physical Education is scheduled at ___________am/pm, Days M T W Th F |
|
Snack: _____is not necessary before PE. |
|
Snack times____________________ Will student need to be reminded? _n/a___yes |
_____no |
Preferred snacks/parent instruction for class parties : Call |
|
parent______________________________________________ |
|
|
|
|
FIELD TRIPS: Extra snacks, glucose monitoring kit, copy of health plan, glucose gel or other emergency supplies must accompany student on field trip.
EMERGENCY RESPONSE PLAN: DIABETES
Student_____________________________DOB____________Grade/Teacher_
Notify parent if child’s blood sugar is below__________or above__________mg/dl.
HYPOGLYCEMIA – INSULIN REACTION (LOW BLOOD SUGAR)
Student to be treated when blood sugar is below ____________________________________
MILD LOW BLOOD SUGAR Signs/Symptoms may include hunger, irritability, shakiness, sleepiness, sweating, pallor, uncooperative, crying or other behavioral changes. Additional student symptoms_______________________________________________________________________
Treatment:
Never leave student unattended. If treated outside the classroom, a responsible person must accompany student to health office.
Give juice (1 carton), or regular pop (1 cup), or 2-3 glucose tabs; (1 small tube of cake decorating gel can also be placed between cheek and gum with head elevated)
Wait 10-15 minutes. Recheck blood sugar. Retreat as above if still below 75, or if symptoms persist.
When symptoms improve or blood sugar is >75, give substantial snack (carbohydrate and protein) or lunch.
Comments:_____________________________________________________________________
SEVERE LOW BLOOD SUGAR:
Signs/Symptoms: Seizure or loss of consciousness or student unwilling/unable to take gel or juice. Treatment:
CALL 911 |
- Stay with student |
Place student on side |
- Do not put anything in mouth |
Comments:________________________________________________________________________
HYPERGLYCEMIA – HIGH BLOOD SUGAR
Student must be treated when blood sugar is above ___________.
Signs/Symptoms may include: extreme thirst, headache, abdominal pain, nausea, increased urination Treatment:
-Drink 6-8 ounces of water every hour. Allow student to carry water bottle with them.
-Use restroom as needed.
-Do not allow exercise.
-Student to administer insulin if ordered by health care provider
-For pumps, will student be able to change infusion set, or have an alternate source of insulin at school?________________________________________________________________________
-If student exhibits nausea, vomiting, stomachache or is lethargic, notify parents and school nurse ASAP.
-Send student back to class if none of the above symptoms are present.
Comments:_______________________________________________________________________
I understand that all monitoring equipment, snacks, glucose are to be provided by the family. In case of an emergency, contact the 911 emergency response team for further evaluation.
If parents are unavailable, the physician or diabetic nurse educator may be contacted for specific information. If transportation by ambulance is necessary, parents will assume responsibility for payment.
Parent(s) Signature:______________________________________ Date:_________________
Nurse Signature:________________________________________ Date:_________________
Confidential