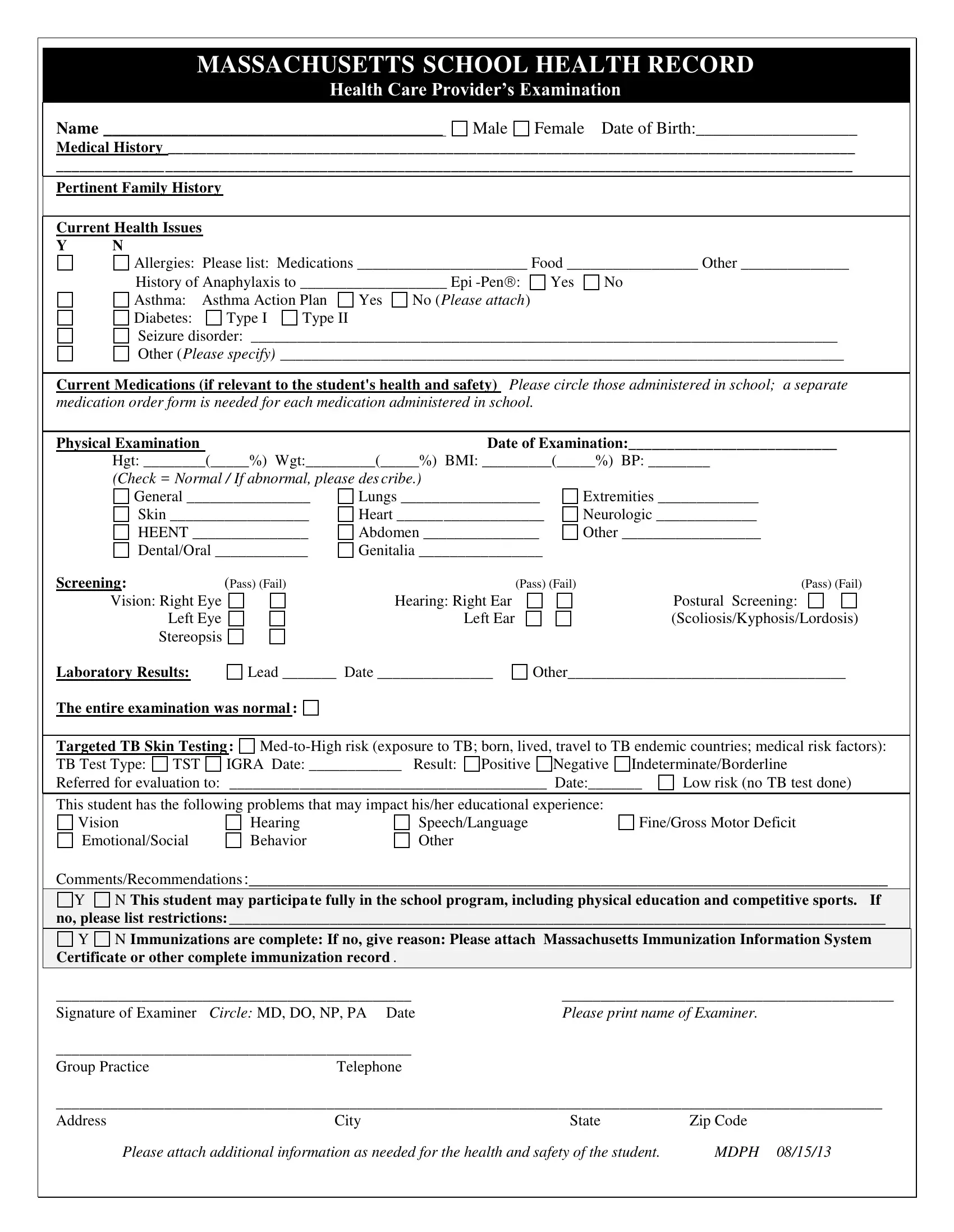
Accommodating a student’s health needs within the educational environment is crucial for their safety, well-being, and academic success. The Massachusetts School Health Record form serves as a comprehensive tool to document and communicate a student's health status, history, and specific medical requirements to school administrators, nurses, and educators. Beginning with the basic identification details, the form captures a wide array of information, including medical history, family health background, current health issues, and allergies, which are vital for understanding potential health risks or necessary interventions. It also inquires about medications, which is essential for those who might need medication during school hours, and outlines whether an Epi-Pen for anaphylaxis or an Asthma Action Plan is required. The form delves into a physical examination summary, showcasing metrics such as height, weight, Body Mass Index (BMI), and blood pressure, along with evaluations of various bodily systems. Vision, hearing, and postural screenings are specifically highlighted to identify issues that could impact a student's educational experience. Furthermore, it addresses the critical aspects of immunizations, ensuring the student meets health requirements for school attendance, and provides space for healthcare providers to recommend participation in school activities or note any restrictions. By gathering and presenting detailed health information, the School Health Record form is fundamental in creating a supportive and informed school environment for every student.
| Question | Answer |
|---|---|
| Form Name | School Health Record Form |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | ma health examination, massachusetts school health form, health provider examination, massachusetts school health |
MASSACHUSETTS SCHOOL HEALTH RECORD
HEALTH CARE PROVIDER’S EXAMINATION
Name ________________________________________ |
Male |
Female Date of Birth:___________________ |
Medical History _________________________________________________________________________________________
_______________________________________________________________________________________________________
Pertinent Family History
|
Current Health Issues |
|
|
|
|
|
|
|
|
|
|
Y |
N |
|
|
|
|
|
|
|
|
|
|
Allergies: Please list: Medications ______________________ Food _________________ Other ______________ |
||||||||
|
|
History of Anaphylaxis to ___________________ Epi |
: |
Yes |
No |
|||||
|
|
Asthma: |
Asthma Action Plan |
Yes |
No (Please attach) |
|
|
|||
|
|
Diabetes: |
Type I |
Type II |
|
|
|
|
|
|
|
|
Seizure disorder: ____________________________________________________________________________ |
||||||||
|
|
Other (Please specify) _________________________________________________________________________ |
||||||||
|
|
|
||||||||
|
Current Medications (if relevant to the student's health and safety) |
|
Please circle those administered in school; a separate |
|||||||
|
medication order form is needed for each medication administered in school. |
|
|
|||||||
Physical Examination |
|
Date of Examination:___________________________ |
|
Hgt: ________(_____%) Wgt:_________(_____%) BMI: _________(_____%) BP: ________ |
|||
(Check = Normal / If abnormal, please des cribe.) |
|
||
General ________________ |
Lungs __________________ |
Extremities _____________ |
|
Skin __________________ |
Heart ___________________ |
Neurologic _____________ |
|
HEENT _______________ |
Abdomen _______________ |
Other __________________ |
|
Dental/Oral ____________ |
Genitalia ________________ |
|
|
Screening: |
|
(Pass) (Fail) |
|
(Pass) (Fail) |
(Pass) (Fail) |
|
Vision: Right Eye |
|
Hearing: Right Ear |
|
Postural Screening: |
||
|
Left Eye |
|
|
Left Ear |
|
(Scoliosis/Kyphosis/Lordosis) |
|
Stereopsis |
|
|
|
|
|
Laboratory Results: |
|
Lead _______ Date _______________ |
Other____________________________________ |
|||
The entire examination was normal : |
|
|
|
|||
|
|
|||||
Targeted TB Skin Testing : |
||||||
TB Test Type: |
TST |
IGRA Date: ____________ Result: |
Positive Negative Indeterminate/Borderline |
|||
Referred for evaluation to: |
_________________________________________ Date:_______ |
Low risk (no TB test done) |
||||
This student has the following problems that may impact his/her educational experience:
Vision |
Hearing |
Speech/Language |
Emotional/Social |
Behavior |
Other |
Fine/Gross Motor Deficit
Comments/Recommendations :_____________________________________________________________________
Y |
N This student may participa te fully in the school program, including physical education and competitive sports. If |
no, please list restrictions: _____________________________________________________________________________________
Y |
N Immunizations are complete: If no, give reason: Please attach Massachusetts Immunization Information System |
||
Certificate or other complete immunization record . |
|
||
______________________________________________ |
___________________________________________ |
||
Signature of Examiner |
Circle: MD, DO, NP, PA Date |
Please print name of Examiner. |
|
______________________________________________ |
|
||
Group Practice |
Telephone |
|
|
___________________________________________________________________________________________________________
Address |
City |
State |
Zip Code |
Please attach additional information as needed for the health and safety of the student. |
MDPH 08/15/13 |