Any person who makes or causes to be made any |
|
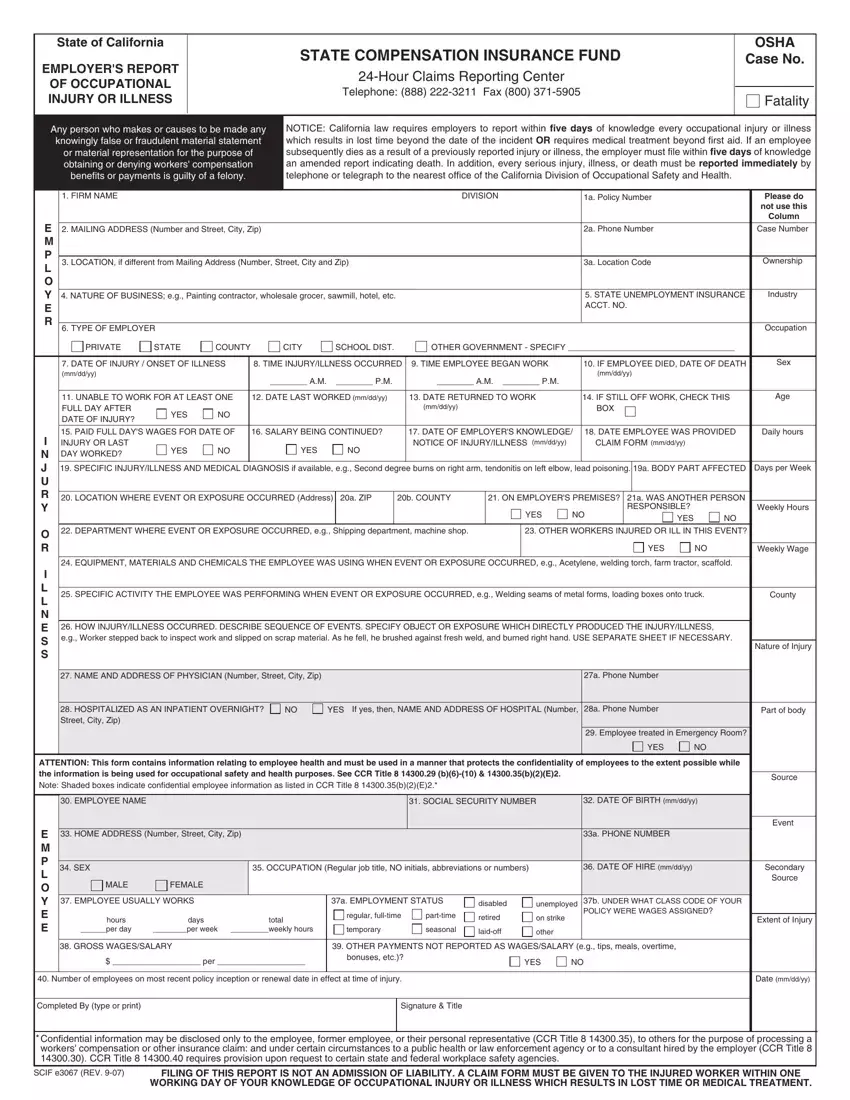
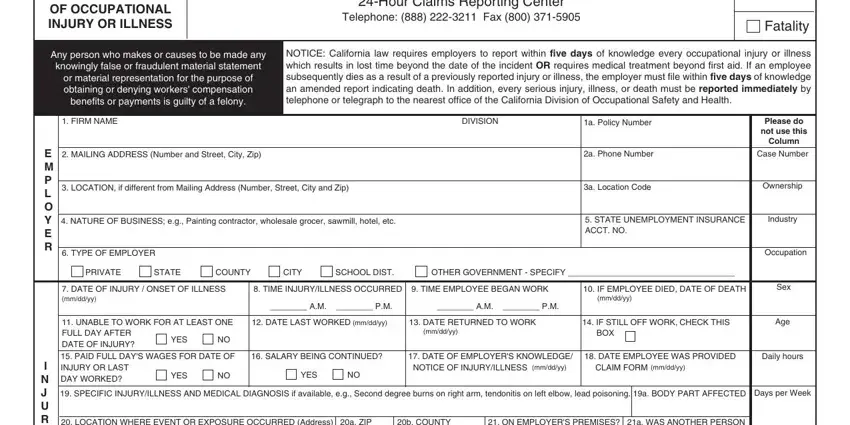
NOTICE: California law requires employers to report within five days of knowledge every occupational injury or illness |
|
knowingly false or fraudulent material statement |
|
which results in lost time beyond the date of the incident OR requires medical treatment beyond first aid. If an employee |
|
|
or material representation for the purpose of |
|
subsequently dies as a result of a previously reported injury or illness, the employer must file within five days of knowledge |
|
|
obtaining or denying workers' compensation |
|
an amended report indicating death. In addition, every serious injury, illness, or death must be reported immediately by |
|
|
benefits or payments is guilty of a felony. |
|
|
telephone or telegraph to the nearest office of the California Division of Occupational Safety and Health. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
1. FIRM NAME |
|
|
|
|
|
|
|
|
DIVISION |
|
|
1a. Policy Number |
|
|
|
Please do |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
not use this |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Column |
E |
2. MAILING ADDRESS (Number and Street, City, Zip) |
|
|
|
|
|
|
|
|
|
|
2a. Phone Number |
|
|
|
Case Number |
M |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
P |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
3. LOCATION, if different from Mailing Address (Number, Street, City and Zip) |
|
|
|
|
|
|
3a. Location Code |
|
|
|
Ownership |
L |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
O |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Y |
4. NATURE OF BUSINESS; e.g., Painting contractor, wholesale grocer, sawmill, hotel, etc. |
|
|
|
|
|
|
5. STATE UNEMPLOYMENT INSURANCE |
Industry |
E |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
ACCT. NO. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
R |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
6. TYPE OF EMPLOYER |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Occupation |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
PRIVATE |
STATE |
COUNTY |
|
CITY |
|
SCHOOL DIST. |
|
OTHER GOVERNMENT - SPECIFY ____________________________________ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
7. DATE OF INJURY / ONSET OF ILLNESS |
8. TIME INJURY/ILLNESS OCCURRED |
9. TIME EMPLOYEE BEGAN WORK |
|
10. IF EMPLOYEE DIED, DATE OF DEATH |
Sex |
|
|
(mm/dd/yy) |
|
|
|
________ A.M. |
|
________ P.M. |
|
|
|
|
|
|
(mm/dd/yy) |
|
|
|
|
|
|
|
|
|
|
|
|
________ A.M. ________ P.M. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
11. UNABLE TO WORK FOR AT LEAST ONE |
12. DATE LAST WORKED (mm/dd/yy) |
|
13. DATE RETURNED TO WORK |
|
14. IF STILL OFF WORK, CHECK THIS |
Age |
|
|
FULL DAY AFTER |
YES |
NO |
|
|
|
|
|
|
(mm/dd/yy) |
|
|
|
|
BOX |
|
|
|
|
|
|
DATE OF INJURY? |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
15. PAID FULL DAY'S WAGES FOR DATE OF |
16. SALARY BEING CONTINUED? |
|
17. DATE OF EMPLOYER'S KNOWLEDGE/ |
18. DATE EMPLOYEE WAS PROVIDED |
Daily hours |
I |
|
INJURY OR LAST |
YES |
NO |
|
|
YES |
|
NO |
|
NOTICE OF INJURY/ILLNESS (mm/dd/yy) |
|
CLAIM FORM (mm/dd/yy) |
|
|
|
N |
|
DAY WORKED? |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
J |
19. SPECIFIC INJURY/ILLNESS AND MEDICAL DIAGNOSIS if available, e.g., Second degree burns on right arm, tendonitis on left elbow, lead poisoning. |
19a. BODY PART AFFECTED |
Days per Week |
U |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
R |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
20. LOCATION WHERE EVENT OR EXPOSURE OCCURRED (Address) |
20a. ZIP |
20b. COUNTY |
|
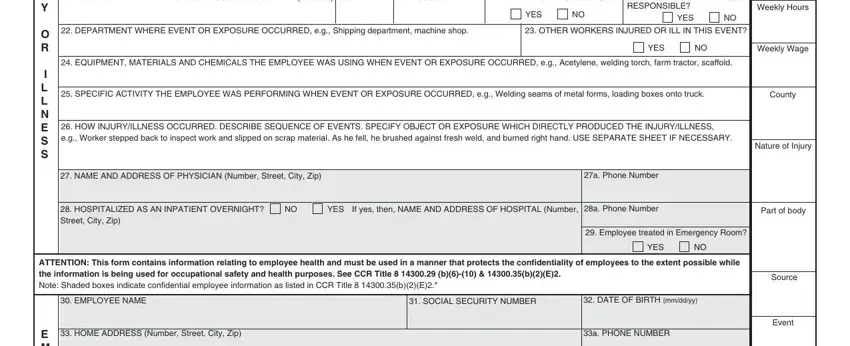
21. ON EMPLOYER'S PREMISES? |
21a. WAS ANOTHER PERSON |
|
Y |
|
|
|
|
|
|
|
|
|
|
|
|
|
YES |
NO |
RESPONSIBLE? |
|
|
Weekly Hours |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
YES |
NO |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
O |
|
22. DEPARTMENT WHERE EVENT OR EXPOSURE OCCURRED, e.g., Shipping department, machine shop. |
|
|
23. OTHER WORKERS INJURED OR ILL IN THIS EVENT? |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
R |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
YES |
|
NO |
Weekly Wage |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
24. EQUIPMENT, MATERIALS AND CHEMICALS THE EMPLOYEE WAS USING WHEN EVENT OR EXPOSURE OCCURRED, e.g., Acetylene, welding torch, farm tractor, scaffold. |
|
I |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
L |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
25. SPECIFIC ACTIVITY THE EMPLOYEE WAS PERFORMING WHEN EVENT OR EXPOSURE OCCURRED, e.g., Welding seams of metal forms, loading boxes onto truck. |
County |
L |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
N |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
E |
|
26. HOW INJURY/ILLNESS OCCURRED. DESCRIBE SEQUENCE OF EVENTS. SPECIFY OBJECT OR EXPOSURE WHICH DIRECTLY PRODUCED THE INJURY/ILLNESS, |
|
S |
|
e.g., Worker stepped back to inspect work and slipped on scrap material. As he fell, he brushed against fresh weld, and burned right hand. USE SEPARATE SHEET IF NECESSARY. |
|
|
Nature of Injury |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
S |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
27. NAME AND ADDRESS OF PHYSICIAN (Number, Street, City, Zip) |
|
|
|
|
|
|
|
|
27a. Phone Number |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
28. HOSPITALIZED AS AN INPATIENT OVERNIGHT? |
|
NO |
YES If yes, then, NAME AND ADDRESS OF HOSPITAL (Number, |
28a. Phone Number |
|
|
|
Part of body |
|
|
Street, City, Zip) |
|
|
|
|
|
|
|
|
(Number, Street, City, Zip) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
29. Employee treated in Emergency Room? |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
YES |
|
NO |
|
|
ATTENTION: This form contains information relating to employee health and must be used in a manner that protects the confidentiality of employees to the extent possible while |
|
the information is being used for occupational safety and health purposes. See CCR Title 8 14300.29 (b)(6)-(10) & 14300.35(b)(2)(E)2. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Source |
Note: Shaded boxes indicate confidential employee information as listed in CCR Title 8 14300.35(b)(2)(E)2.* |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
30. EMPLOYEE NAME |
|
|
|
|
|
|
|
|
31. SOCIAL SECURITY NUMBER |
|
32. DATE OF BIRTH (mm/dd/yy) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Event |
E |
|
33. HOME ADDRESS (Number, Street, City, Zip) |
|
|
|
|
|
|
|
|
|
|
|
33a. PHONE NUMBER |
|
|
|
|
M |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
P |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
34. SEX |
|
|
35. OCCUPATION (Regular job title, NO initials, abbreviations or numbers) |
|
36. DATE OF HIRE (mm/dd/yy) |
|
|
Secondary |
L |
|
|
|
|
|
|
|
MALE |
FEMALE |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Source |
O |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Y |
37. EMPLOYEE USUALLY WORKS |
|
|
|
|
37a. EMPLOYMENT STATUS |
disabled |
unemployed |
37b. UNDER WHAT CLASS CODE OF YOUR |
|
E |
|
|
|
|
|
|
|
|
regular, full-time |
part-time |
retired |
on strike |
|
POLICY WERE WAGES ASSIGNED? |
|
|
hours |
days |
|
|
total |
|
|
Extent of Injury |
|
|
|
|
|
|
|
|
|
|
|
E |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
______per day |
________per week _________weekly hours |
|
temporary |
|
seasonal |
laid-off |
other |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
38. GROSS WAGES/SALARY |
|
|
|
|
39. OTHER PAYMENTS NOT REPORTED AS WAGES/SALARY (e.g., tips, meals, overtime, |
|
|
|
|
|
|
$ ___________________ per ___________________ |
|
bonuses, etc.)? |
|
|
|
YES |
NO |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
40. Number of employees on most recent policy inception or renewal date in effect at time of injury. |
|
|
|
|
|
|
|
|
|
|
|
Date (mm/dd/yy) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Completed By (type or print) |
|
|
|
|
|
|
|
Signature & Title |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
* Confidential information may be disclosed only to the employee, former employee, or their personal representative (CCR Title 8 14300.35), to others for the purpose of processing a workers' compensation or other insurance claim: and under certain circumstances to a public health or law enforcement agency or to a consultant hired by the employer (CCR Title 8 14300.30). CCR Title 8 14300.40 requires provision upon request to certain state and federal workplace safety agencies.