We have used the hard work of our best developers to design the PDF editor you can take advantage of. Our software will help you fill in the form 3067 fill document easily and don’t waste precious time. What you need to undertake is try out the following quick instructions.
Step 1: Click on the "Get Form Here" button.
Step 2: The document editing page is now available. You can add information or manage existing content.
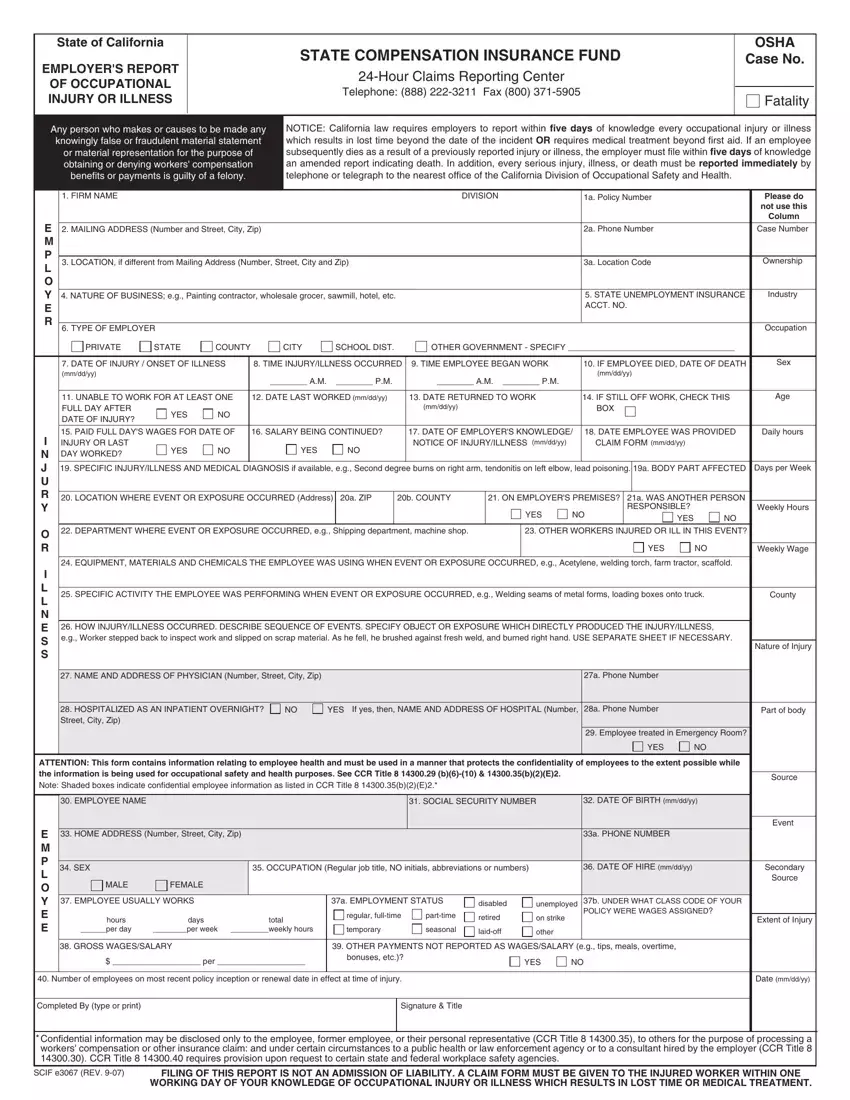
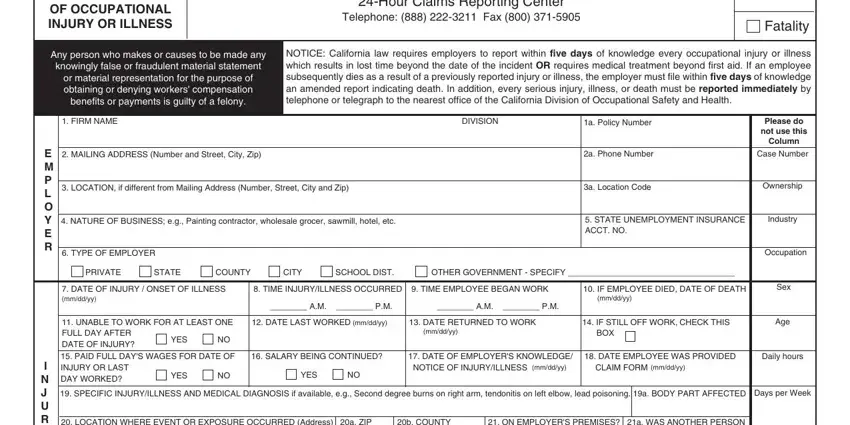
The following parts are within the PDF form you'll be filling out.
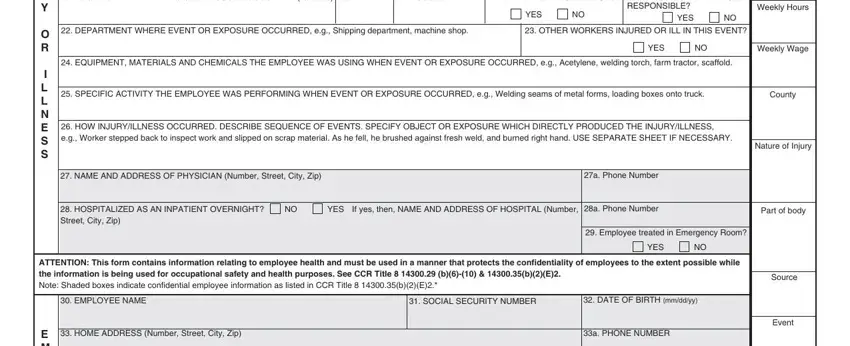
The system will require you to submit the I N J U R Y, O R, I L L N E S S, LOCATION WHERE EVENT OR EXPOSURE, YES NO, RESPONSIBLE, Weekly Hours, YES NO, DEPARTMENT WHERE EVENT OR, OTHER WORKERS INJURED OR ILL IN, EQUIPMENT MATERIALS AND CHEMICALS, YES NO, Weekly Wage, SPECIFIC ACTIVITY THE EMPLOYEE, and County section.
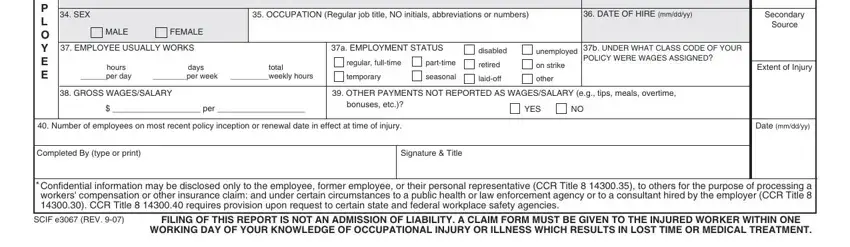
The system will ask for more details with the intention to quickly complete the box E M P L O Y E E, SEX OCCUPATION Regular job title, DATE OF HIRE mmddyy, MALE FEMALE, EMPLOYEE USUALLY WORKS, a EMPLOYMENT STATUS, hours days per day per week weekly, total, regular fulltime, parttime, temporary, seasonal, disabled, unemployed, and retired.
Step 3: After you've selected the Done button, your file should be ready for upload to any electronic device or email address you identify.
Step 4: You can make duplicates of your form toavoid different possible problems. Don't be concerned, we don't disclose or record your information.
