
request advance reimbursement sf can be filled in easily. Just try FormsPal PDF editor to finish the job promptly. Our editor is consistently evolving to deliver the best user experience possible, and that is thanks to our resolve for continuous development and listening closely to customer comments. To start your journey, take these simple steps:
Step 1: Just press the "Get Form Button" in the top section of this webpage to launch our pdf file editing tool. This way, you will find everything that is required to work with your file.
Step 2: After you open the tool, you will find the document all set to be completed. In addition to filling out different blanks, you could also do various other actions with the PDF, including adding any textual content, modifying the initial text, inserting graphics, placing your signature to the document, and a lot more.
As for the blank fields of this precise document, this is what you should do:
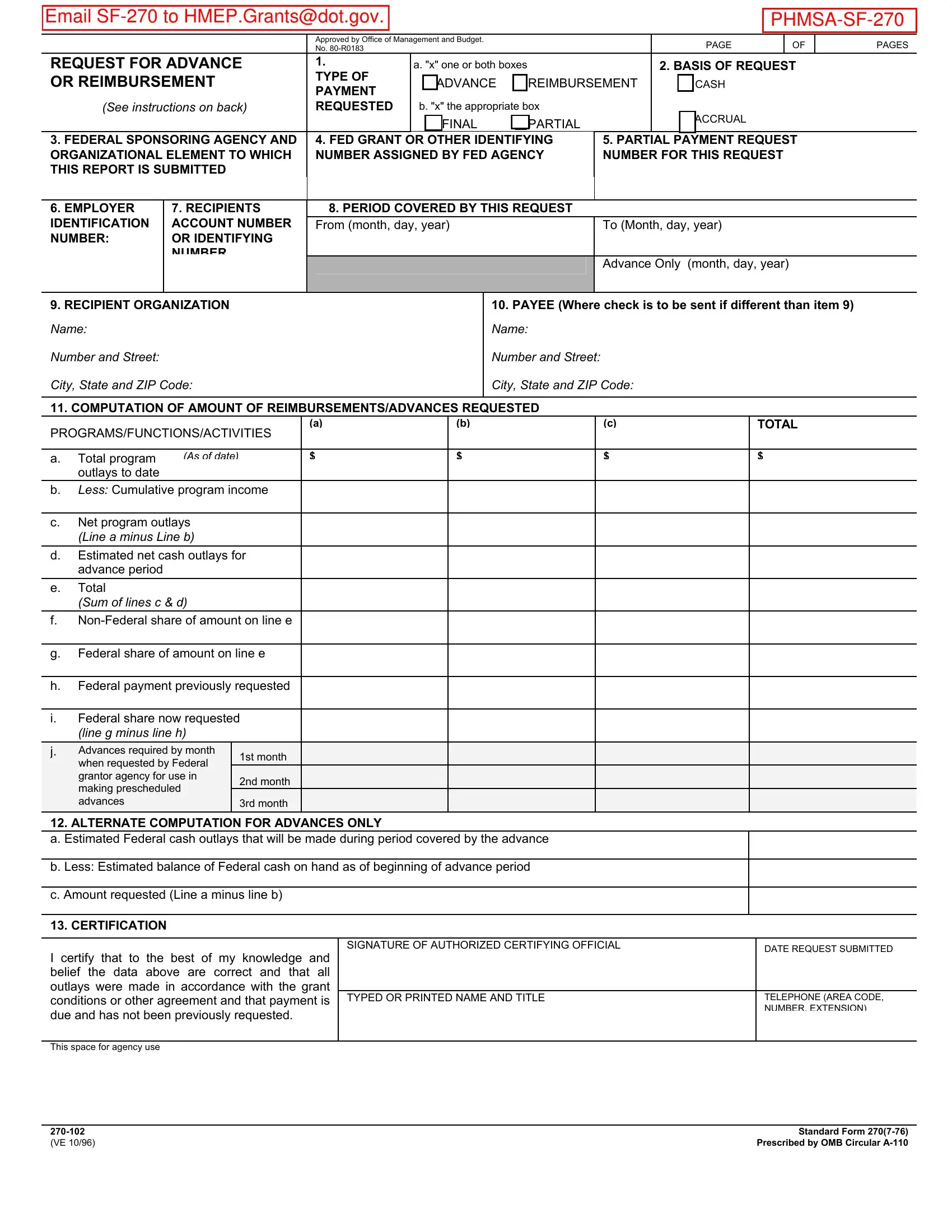
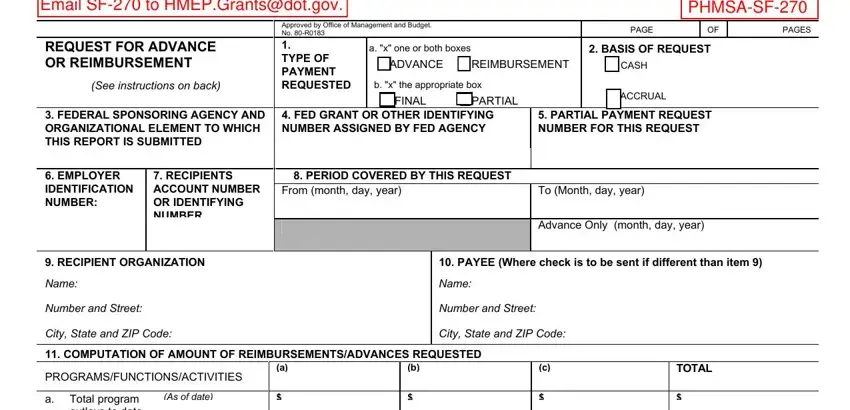
1. First of all, once filling in the request advance reimbursement sf, begin with the part with the next fields:
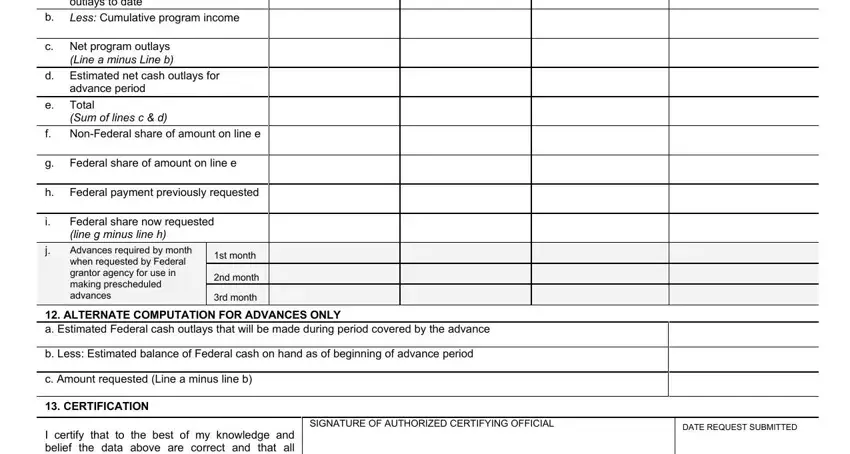
2. After the previous array of fields is done, it's time to put in the essential particulars in a Total program outlays to date, As of date, b Less Cumulative program income, c Net program outlays Line a minus, d Estimated net cash outlays for, advance period, e Total, Sum of lines c d, f NonFederal share of amount on, g Federal share of amount on line e, h Federal payment previously, Federal share now requested line g, Advances required by month when, st month, and nd month so that you can move on to the next part.
A lot of people generally make some mistakes while completing Advances required by month when in this section. Don't forget to review everything you type in here.
3. This third stage is normally straightforward - fill out every one of the blanks in I certify that to the best of my, TYPED OR PRINTED NAME AND TITLE, TELEPHONE AREA CODE NUMBER, This space for agency use, and Standard Form Prescribed by OMB to complete this part.
Step 3: Right after double-checking your entries, press "Done" and you are good to go! Sign up with us now and easily gain access to request advance reimbursement sf, available for download. Every single change made is conveniently saved , letting you edit the form later on anytime. Here at FormsPal.com, we do our utmost to be certain that all your details are stored protected.