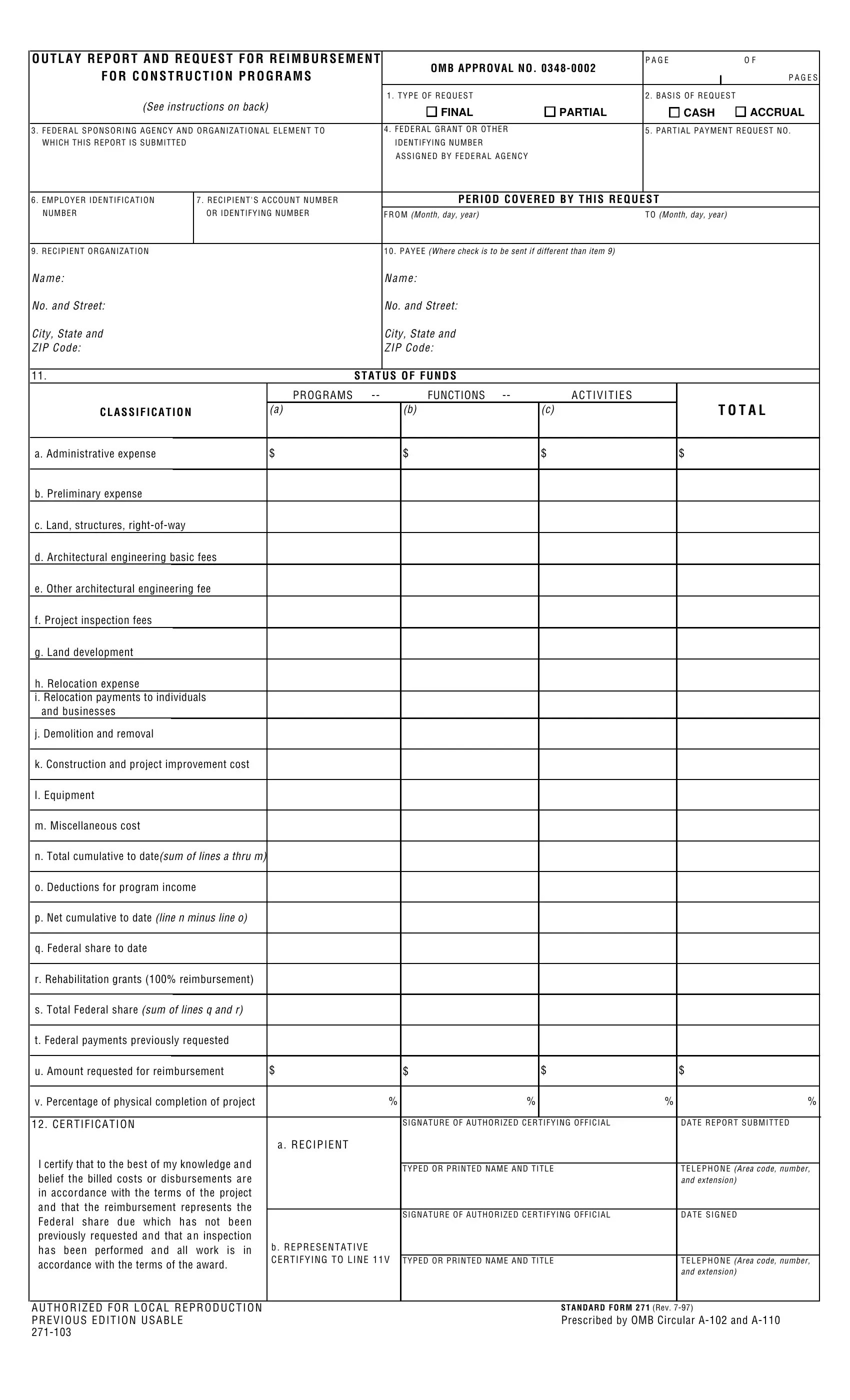
In the realm of federal construction programs, meticulous tracking and reporting of financial expenditures and requests for reimbursement are paramount. This is where the Standard Form 271 (SF 271), also known as the "Outlay Report and Request for Reimbursement for Construction Programs," becomes a critical tool. Devised to ensure transparency and accountability in the management of federal funds, SF 271 serves multiple purposes. It allows grant recipients to report their project expenses and request reimbursement for costs incurred during construction projects sponsored by various federal agencies. The form is comprehensive, covering everything from preliminary and administrative expenses to architectural, engineering, and construction costs. It is designed to accommodate both partial and final requests, based on either cash disbursements or accrued expenditures. Moreover, the form facilitates detailed reporting on the status of funds by categorizing expenditures into specific activities such as land development, relocation expenses, and more. Additionally, it requires certifications by authorized officials, affirming the accuracy and compliance of the reported costs with the grant's terms. The SF 271 is not just a form but a mechanism for ensuring that the spending of federal funds is aligned with the objectives and stipulations of the sponsoring agency, thereby upholding the principles of fiscal responsibility and integrity in government-funded construction projects.
| Question | Answer |
|---|---|
| Form Name | Sf 271 Form |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | form 271, sf271 form fillable, faa 271 form, sf271 |
