
Dealing with PDF files online is always simple with our PDF tool. Anyone can fill out employee call off log template here effortlessly. We are focused on making sure you have the ideal experience with our tool by constantly presenting new functions and improvements. With all of these improvements, using our tool gets better than ever! For anyone who is looking to begin, here's what it's going to take:
Step 1: Hit the "Get Form" button above. It will open our pdf editor so that you can begin completing your form.
Step 2: With the help of this online PDF tool, you are able to do more than merely complete blank fields. Try all of the functions and make your docs look faultless with customized textual content added in, or fine-tune the file's original input to perfection - all that comes along with the capability to incorporate stunning images and sign the PDF off.
It is easy to finish the form using this detailed guide! Here's what you want to do:
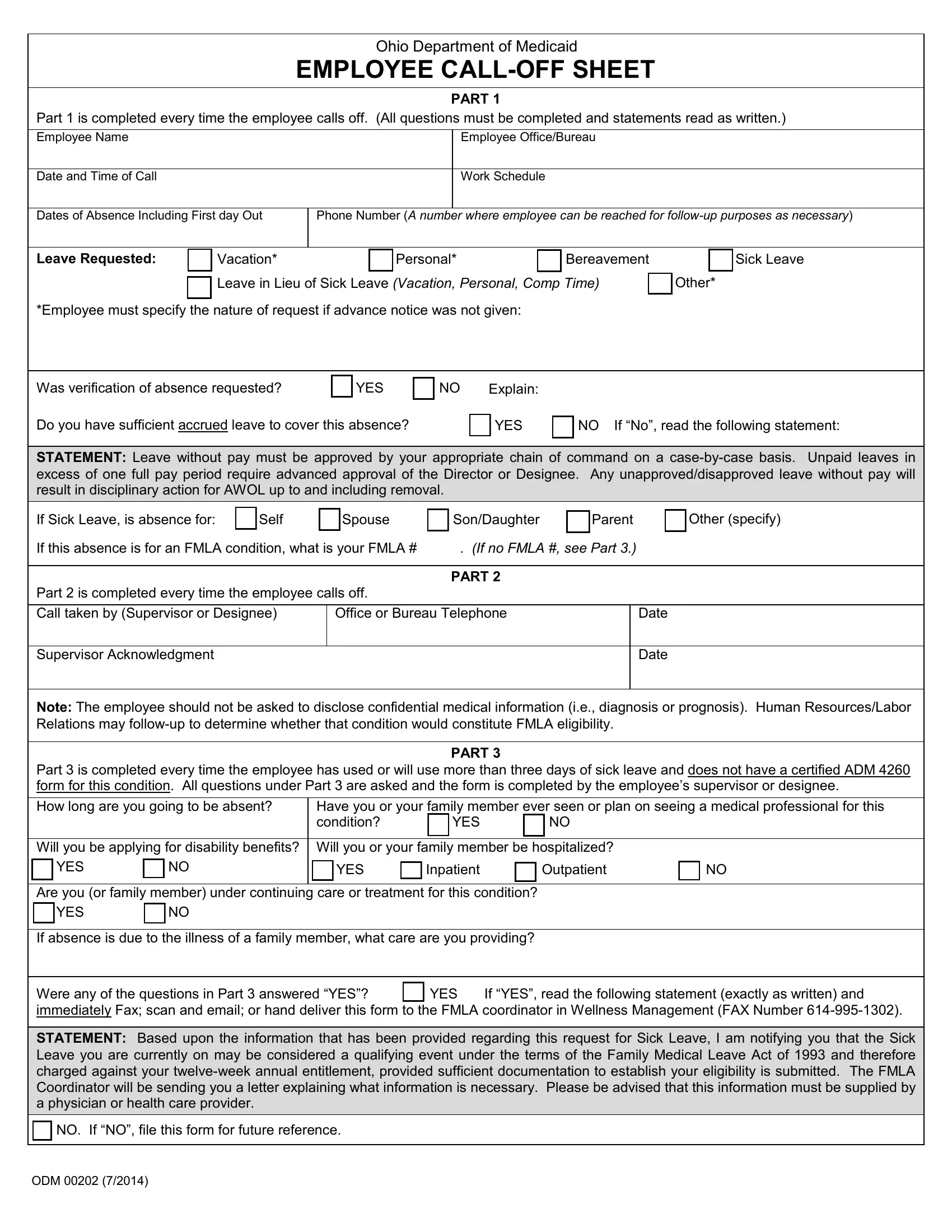
1. The employee call off log template will require specific information to be typed in. Ensure that the following fields are filled out:
2. When the last section is complete, you're ready to insert the needed specifics in Part is completed every time the, Office or Bureau Telephone, Date Date, Note The employee should not be, Part is completed every time the, Have you or your family member, YES, Inpatient, YES, YES, PART, Are you or family member under, YES, If absence is due to the illness, and Were any of the questions in Part in order to progress further.
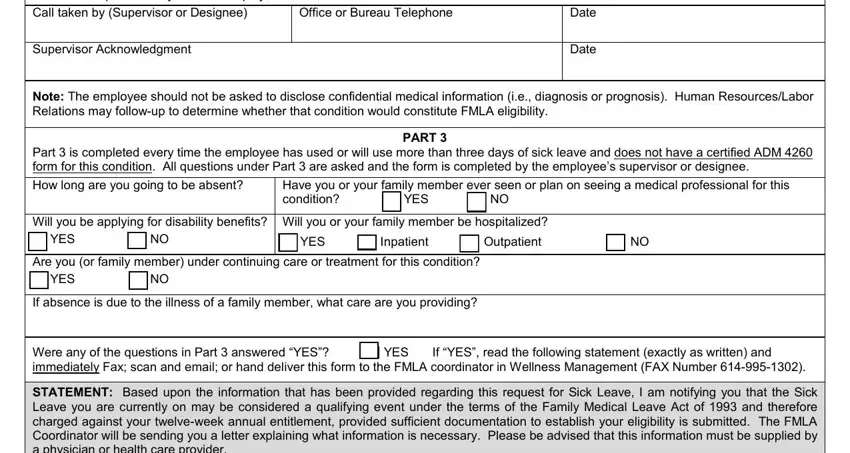
3. This stage will be straightforward - fill in all the empty fields in STATEMENT Based upon the, NO If NO file this form for future, and ODM to conclude this part.

It is easy to make errors while filling out the ODM, therefore be sure to look again prior to deciding to send it in.
Step 3: Just after proofreading the entries, press "Done" and you're all set! Right after getting a7-day free trial account here, it will be possible to download employee call off log template or send it via email directly. The PDF form will also be available via your personal account menu with your each and every modification. FormsPal ensures your information privacy by using a protected system that in no way saves or distributes any kind of personal data involved in the process. Feel safe knowing your docs are kept confidential every time you work with our editor!