We were making the PDF editor with the idea of making it as simple to work with as it can be. That's why the entire process of filling out the soc 821 pdf will likely to be smooth use the next steps:
Step 1: To get started, choose the orange button "Get Form Now".
Step 2: You are now on the document editing page. You can edit, add content, highlight particular words or phrases, put crosses or checks, and put images.
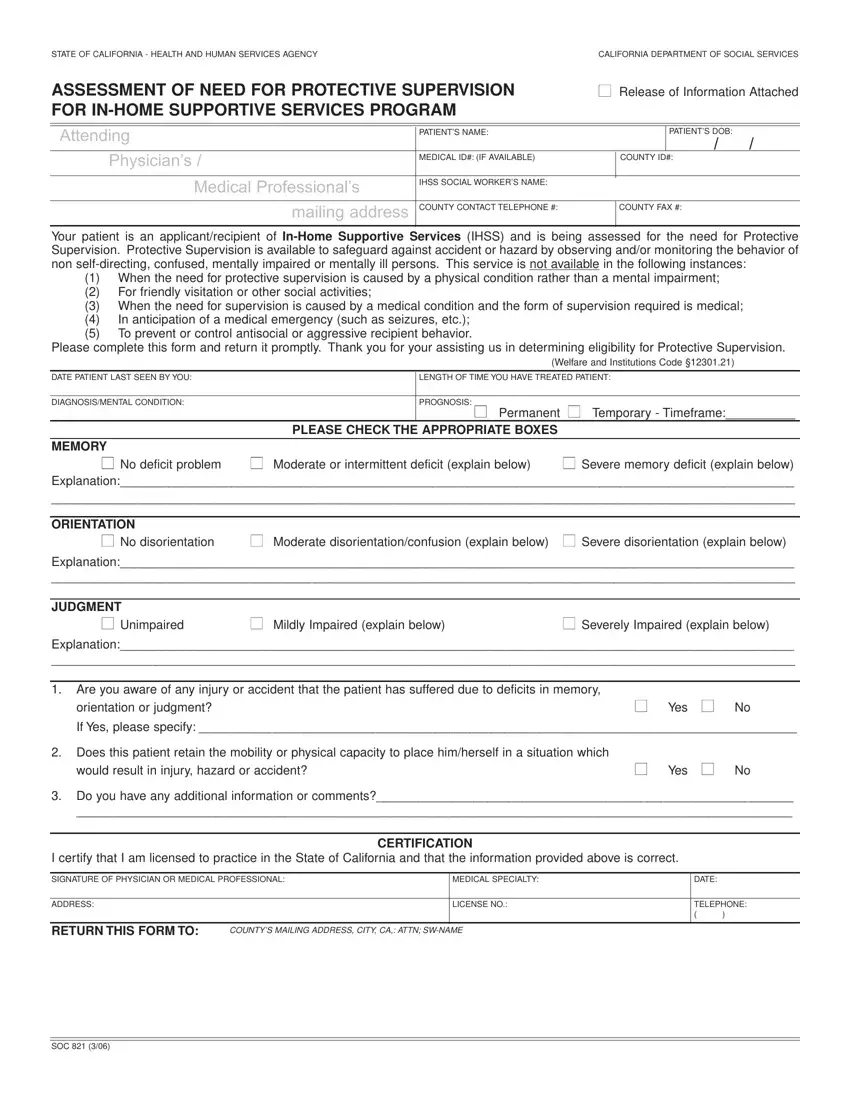
Please type in the next information to create the soc 821 pdf PDF:
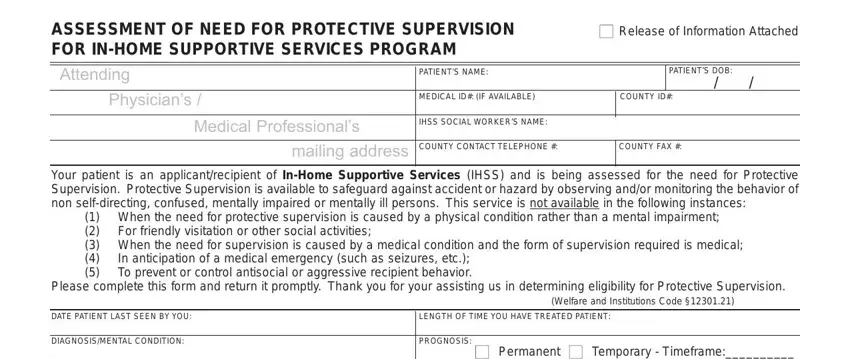
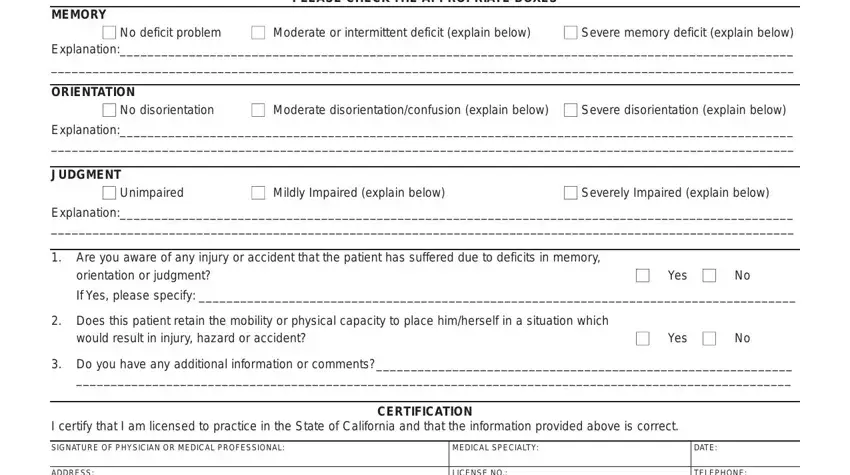
Provide the appropriate data in the space MEMORY, Permanent PLEASE CHECK THE, No deficit problem, Severe memory deficit explain, Moderate or intermittent deficit, ORIENTATION, No disorientation, Moderate disorientationconfusion, Severe disorientation explain below, Explanation, JUDGMENT, Unimpaired, Mildly Impaired explain below, Severely Impaired explain below, and Explanation.
Provide the considerable details the RETURN THIS FORM TO, COUNTYS MAILING ADDRESS CITY, TELEPHONE, and SOC box.
Step 3: When you are done, click the "Done" button to transfer your PDF file.
Step 4: Make sure you keep away from future challenges by preparing no less than 2 duplicates of your form.
