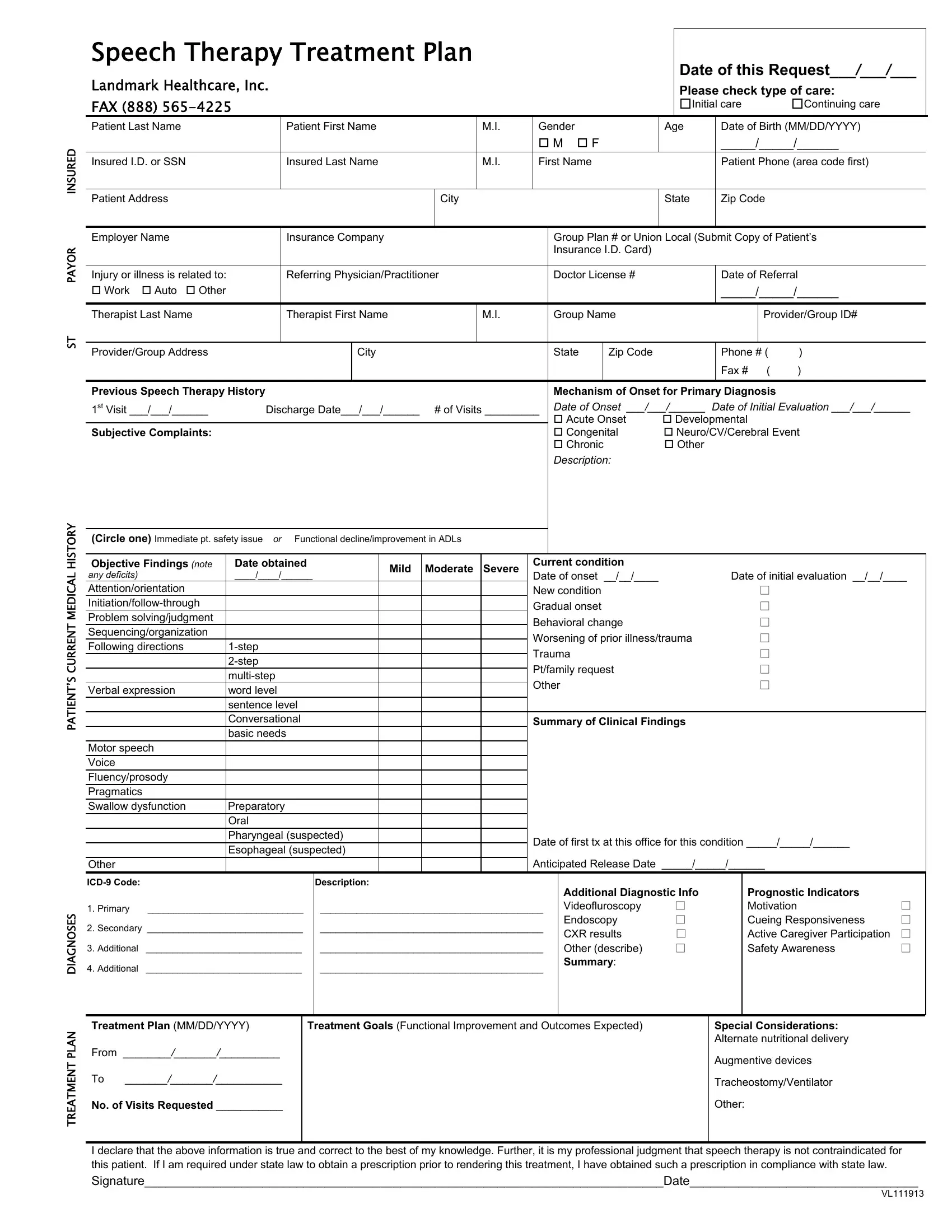
The Speech Therapy Treatment Plan form serves as a foundational bridge connecting patients who are in need of speech therapy services with their healthcare providers, ensuring a structured approach towards diagnosing and treating speech-related disorders. With sections neatly organized to capture essential information, this form begins by soliciting details about the patient's insurance and demographic specifics, such as name, age, and contact information, which are critical for identifying the patient and for billing purposes. The form meticulously outlines the patient's current medical history and the specific diagnosis necessitating speech therapy, underscoring the importance of a thorough understanding of the patient’s health status. It distinguishes between initial and continuing care, highlighting the plan's adaptability to the patient’s evolving needs. The treatment plan section delves into the patient's prior history with speech therapy, if any, and details regarding the onset of the primary diagnosis, facilitating a tailored therapy approach. Objective findings are structured to assess the severity and nature of the speech disorder, guiding therapists in setting realistic treatment goals and anticipated outcomes. Additionally, it requests information on the treatment's expected duration and frequency, enabling a structured timeline for therapy. Importantly, the form also emphasizes the involvement of additional diagnostic tools and prognostic indicators, like patient motivation and caregiver participation, suggesting a holistic approach to treatment planning. By requiring a healthcare provider's signature, the document underscores the accountability and professionalism expected in the treatment planning process, making it a crucial tool for both healthcare providers and patients embarking on a speech therapy journey.
| Question | Answer |
|---|---|
| Form Name | Speech Therapy Treatment Plan Form |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | speech treatment form, speech therapy treatment plan, speech therapy treatment plan sample, speech therapy treatment plan template |
ST PAYOR INSURED
PATIENT’S CURRENT MEDICAL HISTORY
TREATMENT PLAN DIAGNOSES
Speech Therapy Treatment Plan |
|
|
|
|
|
Date of this Request___/___/___ |
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|||||
Landmark Healthcare, Inc. |
|
|
|
|
|
|
|
Please check type of care: |
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|||||
FAX (888) |
|
|
|
|
|
|
|
|
|
|
Initial care |
Continuing care |
||||
Patient Last Name |
|
Patient First Name |
|
M.I. |
Gender |
|
|
Age |
|
Date of Birth (MM/DD/YYYY) |
||||||
|
|
|
|
|
|
|
|
M |
F |
|
|
|
_____/_____/______ |
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
Insured I.D. or SSN |
|
Insured Last Name |
|
M.I. |
First Name |
|
|
|
Patient Phone (area code first) |
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
Patient Address |
|
|
|
City |
|
|
|
|
State |
|
Zip Code |
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|||||
Employer Name |
|
Insurance Company |
|
|
|
Group Plan # or Union Local (Submit Copy of Patient’s |
||||||||||
|
|
|
|
|
|
|
|
Insurance I.D. Card) |
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|||||
Injury or illness is related to: |
|
Referring Physician/Practitioner |
|
Doctor License # |
|
|
|
Date of Referral |
||||||||
Work |
Auto Other |
|
|
|
|
|
|
|
|
|
|
|
|
_____/_____/______ |
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
Therapist Last Name |
|
Therapist First Name |
|
M.I. |
|
Group Name |
|
|
|
|
Provider/Group ID# |
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Provider/Group Address |
|
|
City |
|
|
|
State |
|
Zip Code |
|
|
|
Phone # ( |
) |
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Fax # ( |
) |
|
|
|
|
|
|
|
|
|
|
|
|
||||||
Previous Speech Therapy History |
|
|
|
|
|
|
Mechanism of Onset for Primary Diagnosis |
|
||||||||
1st Visit ___/___/______ |
Discharge Date___/___/______ |
# of Visits _________ Date of Onset ___/___/______ |
Date of Initial Evaluation ___/___/______ |
|||||||||||||
|
|
|
|
|
|
|
|
Acute Onset |
|
Developmental |
|
|||||
Subjective Complaints: |
|
|
|
|
|
|
Congenital |
|
Neuro/CV/Cerebral Event |
|||||||
|
|
|
|
|
|
|
|
Chronic |
|
Other |
|
|
|
|
||
|
|
|
|
|
|
|
|
Description: |
|
|
|
|
|
|
||
(Circle one) Immediate pt. safety issue or Functional decline/improvement in ADLs
Objective Findings (note |
Date obtained |
|
|
Mild |
Moderate |
Severe |
Current condition |
|
|
|
|
|||||
any deficits) |
|
____/____/______ |
|
Date of onset __/__/____ |
|
Date of initial evaluation __/__/____ |
||||||||||
Attention/orientation |
|
|
|
|
|
|
|
New condition |
|
|
□ |
|
||||
|
|
|
|
|
|
|
Gradual onset |
|
|
□ |
|
|||||
Problem solving/judgment |
|
|
|
|
|
|
|
Behavioral change |
|
|
□ |
|
||||
Sequencing/organization |
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
Worsening of prior illness/trauma |
|
□ |
|
||||||
Following directions |
|
|
|
|
|
|
|
|||||||||
|
|
|
|
|
Trauma |
|
|
□ |
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
Pt/family request |
|
|
□ |
|
||||
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
Other |
|
|
|
□ |
|
|||
Verbal expression |
word level |
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
sentence level |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Conversational |
|
|
|
|
|
Summary of Clinical Findings |
|
|
|
||||
|
|
|
basic needs |
|
|
|
|
|
|
|
|
|
|
|
|
|
Motor speech |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
Voice |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Fluency/prosody |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
Pragmatics |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Swallow dysfunction |
Preparatory |
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
Oral |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Pharyngeal (suspected) |
|
|
|
Date of first tx at this office for this condition _____/_____/______ |
|
||||||||
|
|
|
Esophageal (suspected) |
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
Other |
|
|
|
|
|
|
|
|
|
Anticipated Release Date _____/_____/______ |
|
|||||
|
|
|
|
Description: |
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
Additional Diagnostic Info |
|
Prognostic Indicators |
|
|
1. Primary |
______________________________ |
|
___________________________________________ |
|
Videofluroscopy |
□ |
|
Motivation |
□ |
|||||||
2. Secondary ______________________________ |
|
___________________________________________ |
|
Endoscopy |
□ |
|
Cueing Responsiveness |
□ |
||||||||
|
|
CXR results |
□ |
|
Active Caregiver Participation |
□ |
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
3. Additional |
______________________________ |
|
|
___________________________________________ |
|
Other (describe) |
□ |
|
Safety Awareness |
□ |
||||||
4. Additional |
______________________________ |
|
|
___________________________________________ |
|
Summary: |
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
||||||||
Treatment Plan (MM/DD/YYYY) |
|
Treatment Goals (Functional Improvement and Outcomes Expected) |
|
Special Considerations: |
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Alternate nutritional delivery |
|
|
From ________/_______/__________ |
|
|
|
|
|
|
|
|
|
|
Augmentive devices |
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
To |
_______/_______/___________ |
|
|
|
|
|
|
|
|
|
|
Tracheostomy/Ventilator |
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
No. of Visits Requested ___________ |
|
|
|
|
|
|
|
|
|
|
Other: |
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
I declare that the above information is true and correct to the best of my knowledge. Further, it is my professional judgment that speech therapy is not contraindicated for this patient. If I am required under state law to obtain a prescription prior to rendering this treatment, I have obtained such a prescription in compliance with state law.
Signature___________________________________________________________________________Date_________________________________
VL111913