
We've applied the efforts of our best computer programmers to make the PDF editor you intend to operate. Our application will allow you to fill in the social security form ssa 1724 f4 form without any difficulty and don’t waste precious time. Everything you need to undertake is stick to these straightforward actions.
Step 1: Choose the button "Get form here" to open it.
Step 2: So you will be on the file edit page. You can add, alter, highlight, check, cross, include or erase areas or phrases.
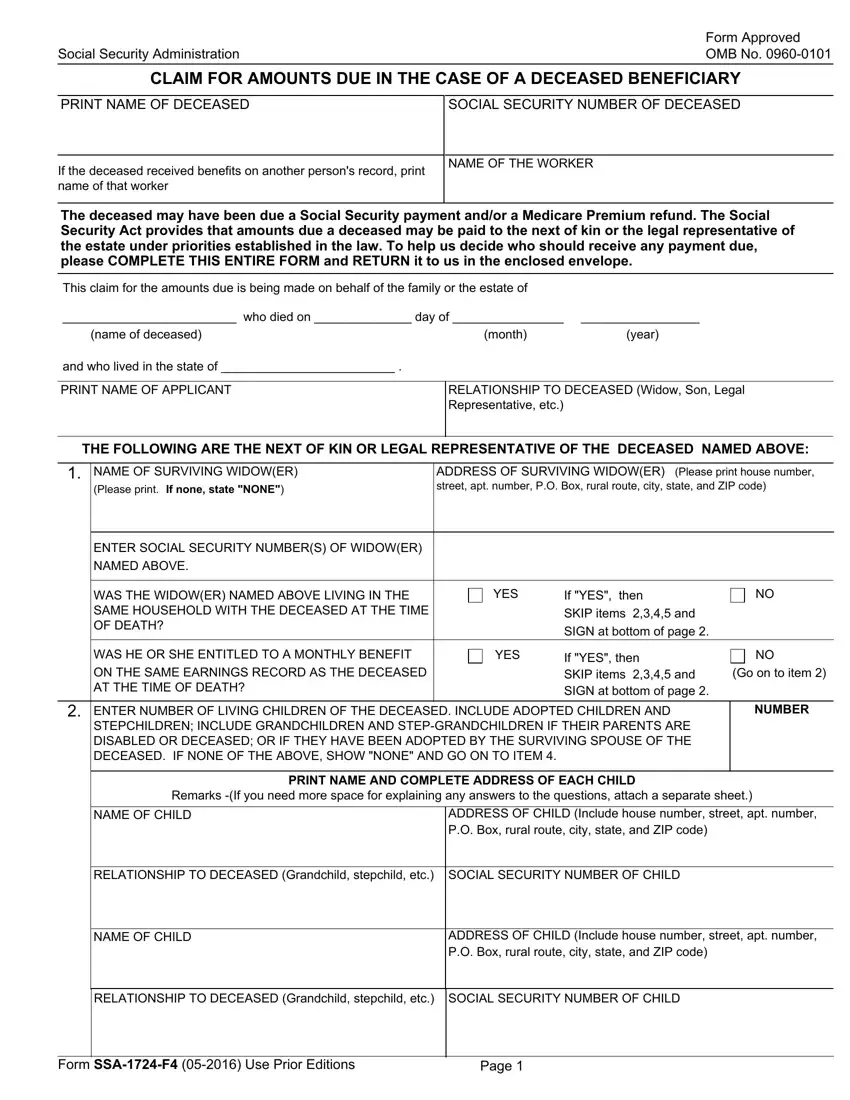
Feel free to provide the following details to fill out the social security form ssa 1724 f4 PDF:
You should provide the information within the box WAS THE WIDOWER NAMED ABOVE LIVING, WAS HE OR SHE ENTITLED TO A, YES, If YES then SKIP items and SIGN, If YES then SKIP items and SIGN, ENTER NUMBER OF LIVING CHILDREN, STEPCHILDREN INCLUDE GRANDCHILDREN, Go on to item, NUMBER, PRINT NAME AND COMPLETE ADDRESS OF, NAME OF CHILD, ADDRESS OF CHILD Include house, RELATIONSHIP TO DECEASED, NAME OF CHILD, and ADDRESS OF CHILD Include house.
Highlight the most vital details the If any child listed in item has a, ENTER NUMBER OF LIVING PARENTS OF, NUMBER, Include adopting parents and, PRINT NAME AND COMPLETE ADDRESS OF, NAME OF LIVING PARENT, ADDRESS OF LIVING PARENT Include, ENTER SOCIAL SECURITY NUMBER OF, NAME OF LIVING PARENT, ADDRESS OF LIVING PARENT Include, ENTER SOCIAL SECURITY NUMBER OF, LEGAL REPRESENTATIVE OF THE, NAME OF LEGAL REPRESENTATIVE, and ADDRESS OF LEGAL REPRESENTATIVE field.
The field ADDRESS OF LEGAL REPRESENTATIVE, NOTE If you are applying as legal, I declare under penalty of perjury, SIGNATURE First name middle, DATE Month day year, SIGNATURE OF APPLICANT, TELEPHONE NUMBER Include area code, MAILING ADDRESS House number and, CITY, STATE, NAME OF COUNTY, ZIP CODE, Direct Deposit Payment Address, Type of Account, and Checking is going to be for you to insert all sides' rights and responsibilities.
Finish by analyzing these sections and filling in the required data: SIGNATURE OF WITNESS, SIGNATURE OF WITNESS, ADDRESS House number and street, ADDRESS House number and street, Form SSAF, and Page.

Step 3: Click the Done button to save your file. Now it is available for upload to your electronic device.
Step 4: To prevent yourself from any kind of concerns in the long run, you should get around two or three duplicates of the form.
