
In case you desire to fill out form ha 4631, you won't have to download any applications - just give a try to our online PDF editor. FormsPal team is always endeavoring to enhance the editor and insure that it is even better for clients with its cutting-edge features. Take advantage of the latest revolutionary possibilities, and discover a trove of new experiences! Here is what you would need to do to start:
Step 1: Access the PDF file in our editor by pressing the "Get Form Button" at the top of this page.
Step 2: The tool provides you with the capability to change your PDF form in a variety of ways. Change it by writing your own text, adjust what's originally in the document, and put in a signature - all close at hand!
Pay close attention while filling in this form. Make sure that all required blanks are filled out accurately.
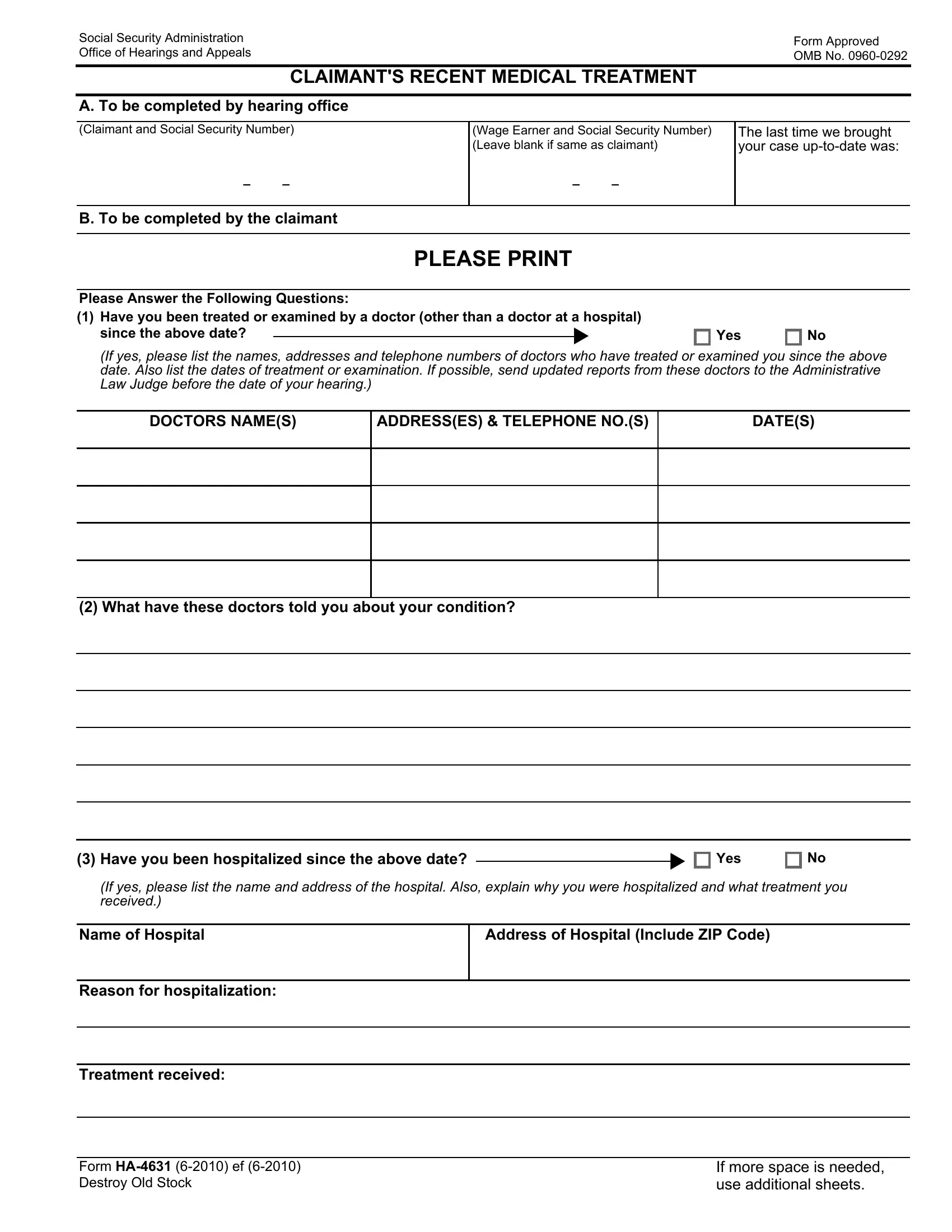
1. Whenever filling in the form ha 4631, be certain to include all needed fields in its associated section. It will help to expedite the work, which allows your details to be handled efficiently and correctly.
2. Your next step is usually to fill out these particular fields: Have you been hospitalized since, u Yes, If yes please list the name and, Name of Hospital, Address of Hospital Include ZIP, Reason for hospitalization, and Treatment received.
It's very easy to make errors while completing your Name of Hospital, so make sure that you reread it prior to deciding to finalize the form.
Step 3: Glance through all the details you've entered into the form fields and then click on the "Done" button. After setting up afree trial account here, you'll be able to download form ha 4631 or email it right away. The file will also be at your disposal in your personal cabinet with your each and every edit. Here at FormsPal, we do everything we can to make certain that all of your information is stored private.