
In case you wish to fill out sss sickness reimbursement form, there's no need to install any programs - simply give a try to our online PDF editor. Our editor is consistently evolving to present the very best user experience possible, and that is because of our commitment to continuous improvement and listening closely to user feedback. Getting underway is effortless! Everything you need to do is follow these basic steps directly below:
Step 1: Hit the "Get Form" button in the top section of this page to open our PDF editor.
Step 2: With our handy PDF editing tool, you may do more than simply fill out forms. Try all of the functions and make your forms appear perfect with custom textual content added, or adjust the file's original content to excellence - all that comes with the capability to insert any type of photos and sign it off.
With regards to the blanks of this particular document, here's what you want to do:
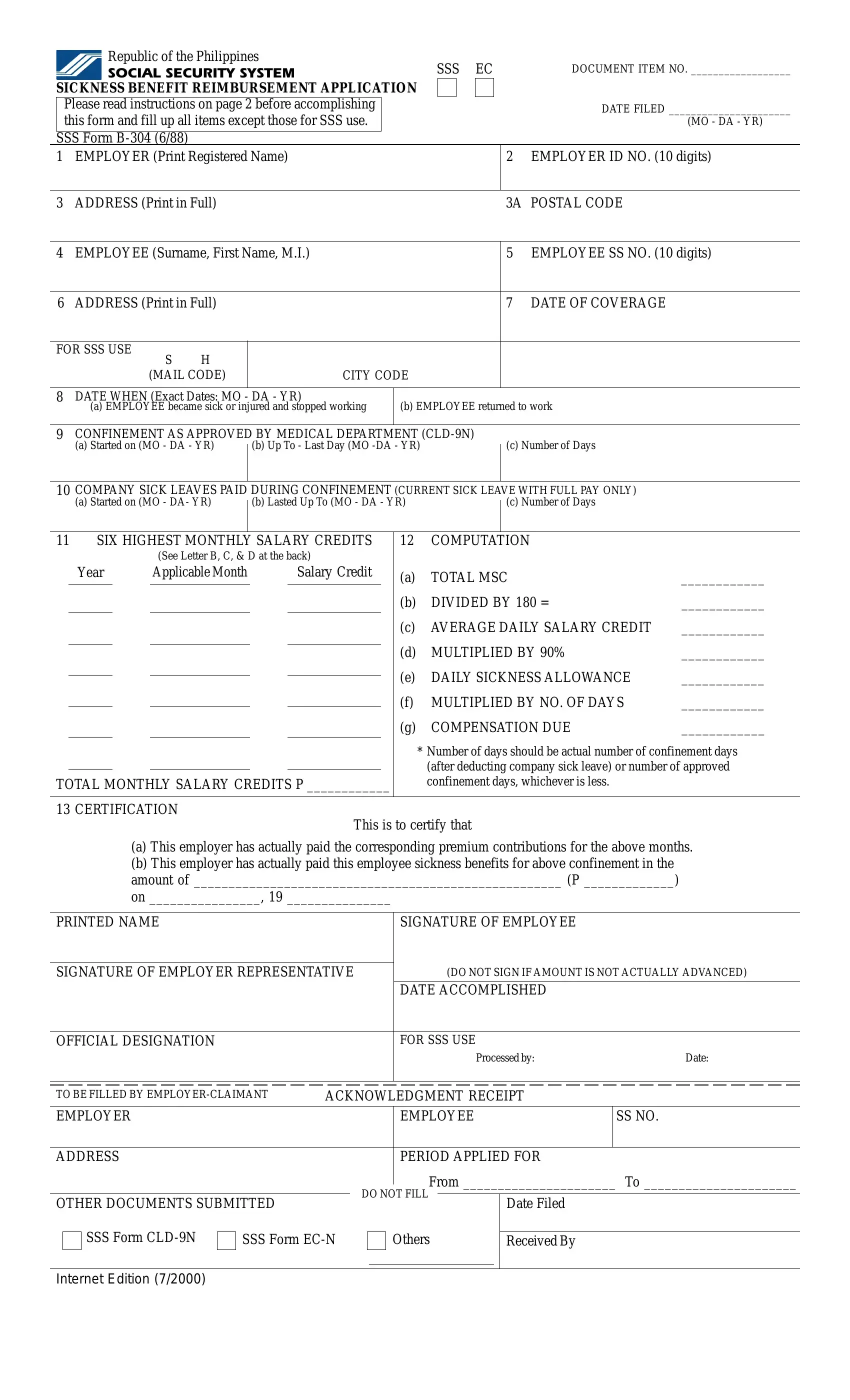
1. It is important to fill out the sss sickness reimbursement form correctly, hence pay close attention while filling in the segments that contain these specific blank fields:
2. Soon after the previous part is done, go on to enter the suitable details in these: COMPANY SICK LEAVES PAID DURING, c Number of Days, a Started on MO DA YR, b Lasted Up To MO DA YR, SIX HIGHEST MONTHLY SALARY CREDITS, COMPUTATION, Year, See Letter B C D at the back, Salary Credit, TOTAL MONTHLY SALARY CREDITS P, CERTIFICATION, TOTAL MSC, DIVIDED BY, AVERAGE DAILY SALARY CREDIT, and MULTIPLIED BY.
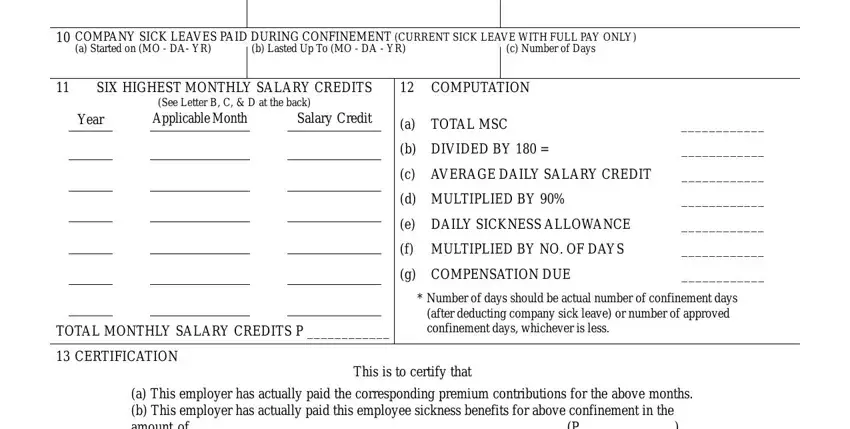
Be really careful when completing SIX HIGHEST MONTHLY SALARY CREDITS and See Letter B C D at the back, as this is where a lot of people make a few mistakes.
3. Through this stage, have a look at a This employer has actually paid, PRINTED NAME, SIGNATURE OF EMPLOYEE, SIGNATURE OF EMPLOYER, DO NOT SIGN IF AMOUNT IS NOT, DATE ACCOMPLISHED, OFFICIAL DESIGNATION, FOR SSS USE, Processed by, Date, TO BE FILLED BY EMPLOYERCLAIMANT, ACKNOWLEDGMENT RECEIPT, EMPLOYEE, SS NO, and ADDRESS. Each one of these should be taken care of with highest attention to detail.
Step 3: Prior to finalizing your form, ensure that all form fields are filled in the right way. When you think it's all good, press “Done." Make a 7-day free trial subscription at FormsPal and get direct access to sss sickness reimbursement form - which you can then work with as you would like from your FormsPal account page. We do not sell or share any information that you use while filling out documents at FormsPal.