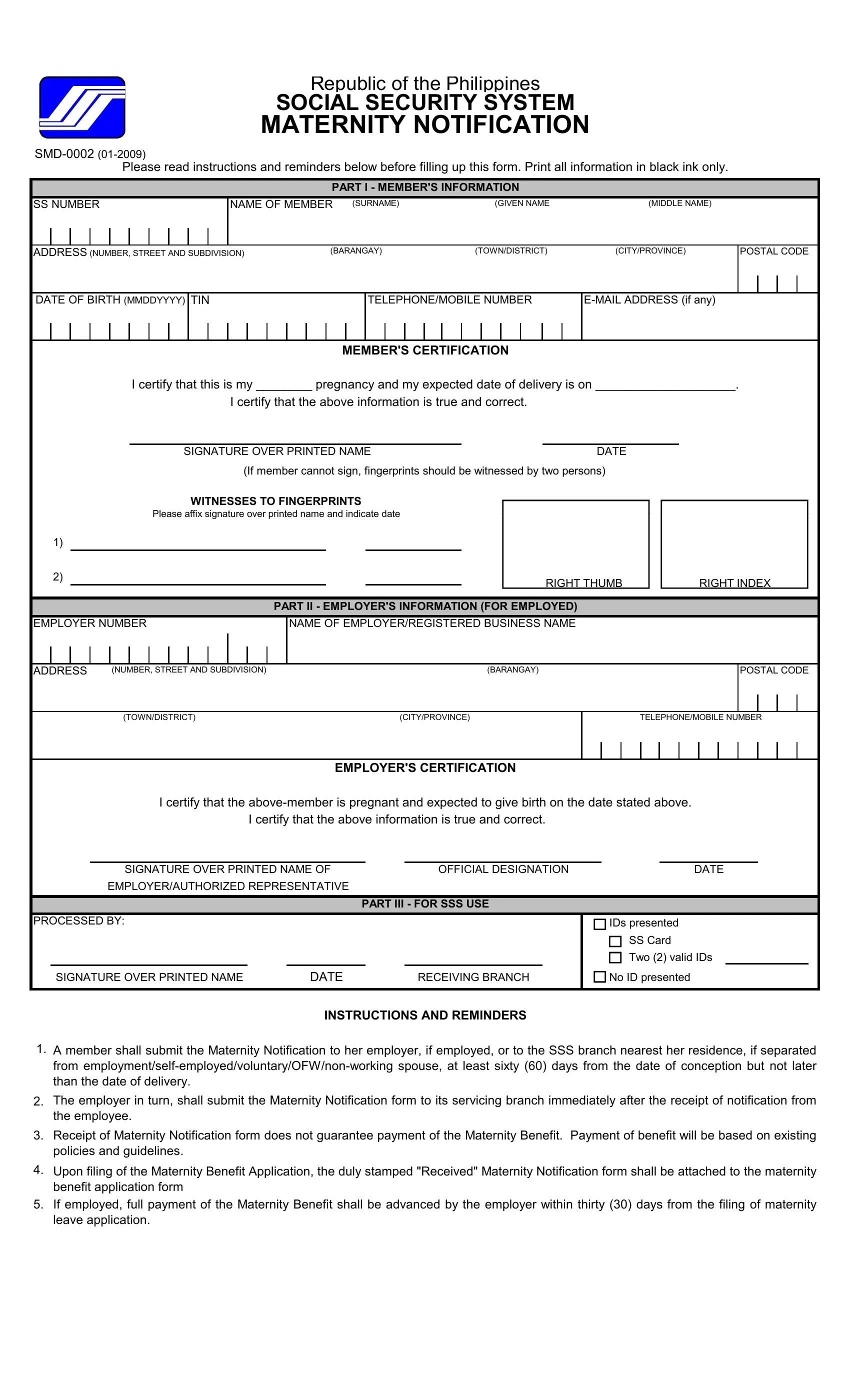
Navigating through pregnancy involves not just health considerations but also financial and administrative planning. One essential step for expectant mothers in the Philippines is the completion of the Social Security System (SSS) Maternity Notification Form, identified formally as SMD-0002. This document facilitates the process for claiming maternity benefits, ensuring support during a crucial period. Designed to be filled out with black ink, the form constitutes three primary sections: member's information, employer's information (for the employed), and a section dedicated to SSS use. Expectant mothers are required to declare their pregnancy, providing crucial details such as their Social Security number, name, address, birth date, and the expected date of delivery, among other personal information. Employers also play a critical role by certifying the pregnancy of their employed members, thus acknowledging the upcoming maternity leave and benefit claims. The form underscores the necessity of early submission - at least sixty days from conception but no later than the date of delivery. Yet, submission of this document does not automatically guarantee the disbursement of benefits, as this is contingent upon adherence to existing policies and guidelines. Furthermore, for employed members, the employer is mandated to advance the full maternity benefit within thirty days from the application for maternity leave, streamlining the process for the expectant mother. Detailed instructions and reminders provided with the form aim to assist in the accurate and timely submission, ensuring all parties involved are well-informed of their roles and responsibilities in the process.
| Question | Answer |
|---|---|
| Form Name | SSS Maternity Notification Form |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | mat 1 form 2021 application, sss mat 1 form 2021, sss mat 1 form 2020 downloadable, mat 1 form |
Republic of the Philippines
SOCIAL SECURITY SYSTEM
MATERNITY NOTIFICATION
Please read instructions and reminders below before filling up this form. Print all information in black ink only.
PART I - MEMBER'S INFORMATION
SS NUMBER
NAME OF MEMBER (SURNAME) |
(GIVEN NAME |
(MIDDLE NAME) |
ADDRESS (NUMBER, STREET AND SUBDIVISION) |
(BARANGAY) |
(TOWN/DISTRICT) |
(CITY/PROVINCE) |
POSTAL CODE
DATE OF BIRTH (MMDDYYYY) TIN
TELEPHONE/MOBILE NUMBER
MEMBER'S CERTIFICATION
I certify that this is my ________ pregnancy and my expected date of delivery is on ____________________.
I certify that the above information is true and correct.
|
SIGNATURE OVER PRINTED NAME |
DATE |
|
||
|
(If member cannot sign, fingerprints should be witnessed by two persons) |
|
|||
|
WITNESSES TO FINGERPRINTS |
|
|
||
|
Please affix signature over printed name and indicate date |
|
|
||
1) |
|
|
|
|
|
2) |
|
|
|
RIGHT THUMB |
RIGHT INDEX |
|
|
|
|
||
PART II - EMPLOYER'S INFORMATION (FOR EMPLOYED)
EMPLOYER NUMBER
NAME OF EMPLOYER/REGISTERED BUSINESS NAME
ADDRESS |
(NUMBER, STREET AND SUBDIVISION) |
(BARANGAY) |
POSTAL CODE
(TOWN/DISTRICT) |
(CITY/PROVINCE) |
TELEPHONE/MOBILE NUMBER
EMPLOYER'S CERTIFICATION
I certify that the
I certify that the above information is true and correct.
|
SIGNATURE OVER PRINTED NAME OF |
OFFICIAL DESIGNATION |
DATE |
|
EMPLOYER/AUTHORIZED REPRESENTATIVE |
|
|
|
|
|
|
|
|
PART III - FOR SSS USE |
|
|
|
|
|
PROCESSED BY:
SIGNATURE OVER PRINTED NAME |
DATE |
RECEIVING BRANCH |
IDs presented
SS Card
Two (2) valid IDs No ID presented
INSTRUCTIONS AND REMINDERS
1.A member shall submit the Maternity Notification to her employer, if employed, or to the SSS branch nearest her residence, if separated from
2.The employer in turn, shall submit the Maternity Notification form to its servicing branch immediately after the receipt of notification from the employee.
3.Receipt of Maternity Notification form does not guarantee payment of the Maternity Benefit. Payment of benefit will be based on existing policies and guidelines.
4.Upon filing of the Maternity Benefit Application, the duly stamped "Received" Maternity Notification form shall be attached to the maternity benefit application form
5.If employed, full payment of the Maternity Benefit shall be advanced by the employer within thirty (30) days from the filing of maternity leave application.