Writing the health benefits form document is a breeze using our PDF editor. Keep up with these actions to obtain the document in a short time.
Step 1: Hit the orange "Get Form Now" button on the website page.
Step 2: At this point, you are on the document editing page. You may add information, edit current information, highlight certain words or phrases, insert crosses or checks, insert images, sign the template, erase unneeded fields, etc.
Prepare the next segments to fill out the template:
Provide the requested particulars in the Annuitants Who Cancel Their, Part G Suspension of FEHB CSRS, Generally you cannot reenroll as, If you cancel your enrollment for, Former Spouses Spouse Equity Who, If you cancel your enrollment for, Place an X in the box only if you, You may suspend your FEHB, for the needy, TRICARE including Uniformed, TRICARE for Life, CHAMPVA or Peace Corps, You can reenroll in the FEHB, and You must submit documentation of section.
You can be demanded specific relevant particulars to be able to complete the Pursuant to USC a e this Privacy, Public Burden Statement We, and Standard Form Revised November area.
For paragraph Premium Conversion allows, Qualifying Life Events QLEs that, Change that May Be Permitted, Premium Conversion Change that May, Time Limits in which Change May Be, Event Code, Event, From Not Enrolled To Enrolled, From Self Only to Self Plus One or, From One Plan or Option to Another, Cancel or Change to Self Plus One, Switch Designated Family Member, Participate, Waive, and When You Must File Health Benefits, state the rights and responsibilities.
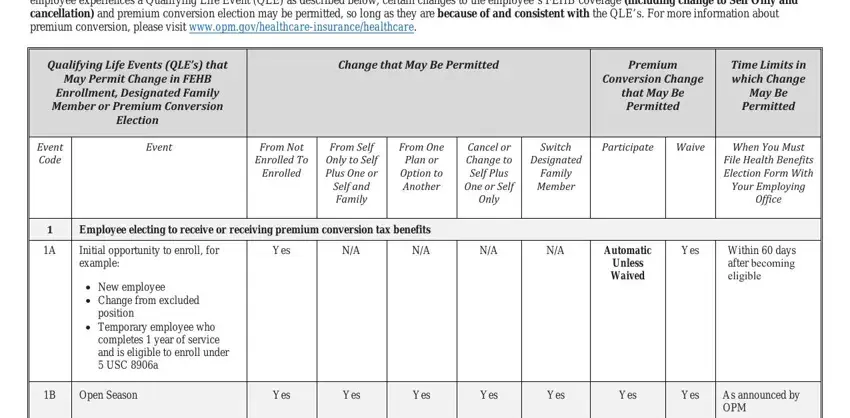
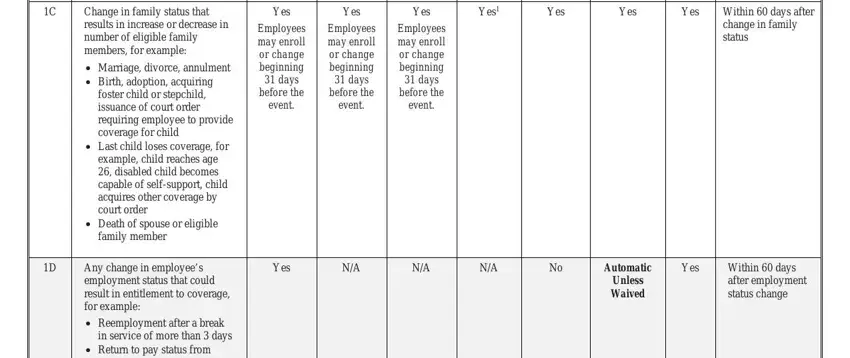
Complete the file by taking a look at all these sections: Yes, Yes, Yes, Yes, Yes, Yes, Yes, Employees may enroll or change, Employees may enroll or change, Employees may enroll or change, Within days after change in, Yes, Automatic Unless Waived, Yes, and Within days after employment.
Step 3: As soon as you've hit the Done button, your form should be readily available upload to any gadget or email address you indicate.
Step 4: Make duplicates of your document. This may prevent future difficulties. We do not watch or disclose your data, so be sure it will be protected.
