




This PDF editor allows you to create forms. There's no need to do much to update Supplemental Questionnaire for Selected Positions - OPM forms. Only stick to the following actions.
Step 1: Click on the button "Get Form Here".
Step 2: The file editing page is now open. It's possible to add information or manage current data.
The following sections will constitute the PDF document that you'll be filling in:
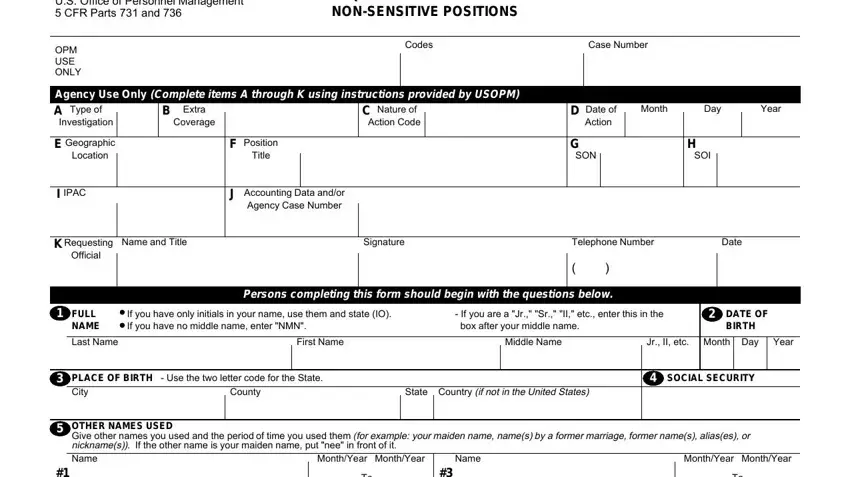
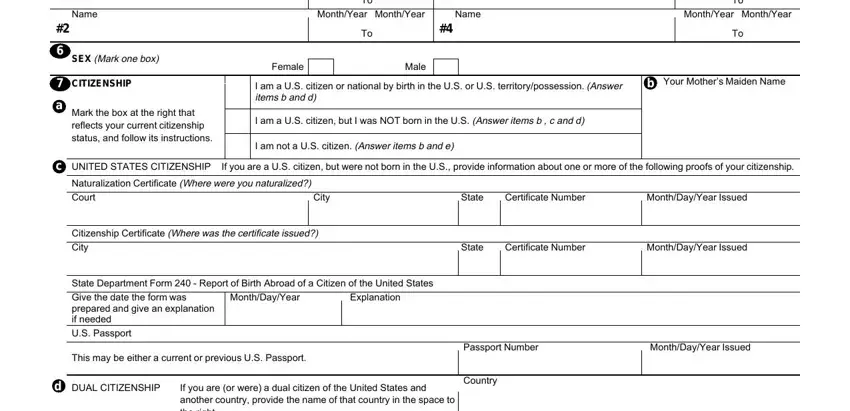
Make sure you submit the Name, SEX Mark onebox, CITIZENSHIP, Mark the box at the right that, MonthYear, MonthYear, Name, MonthYear, MonthYear, Female, Male, I am a US citizen or national by, b Your Mothers Maiden Name, I am a US citizen but I was NOT, and I am not a US citizen Answer items box with the necessary particulars.
Note all data you need in the field Place You Entered the United States, City, State Date You Entered US, Alien Registration Number, Countryies of Citizenship, Month, Day, Year, and Page.

The area MonthYear, MonthYear, Street Address, Apt City Country, State, ZIP Code, Present Name of Person Who Knows, Street Address, Apt City Country, State, ZIP Code, MonthYear, MonthYear, Street Address, and Apt City Country will be for you to put each side's rights and obligations.
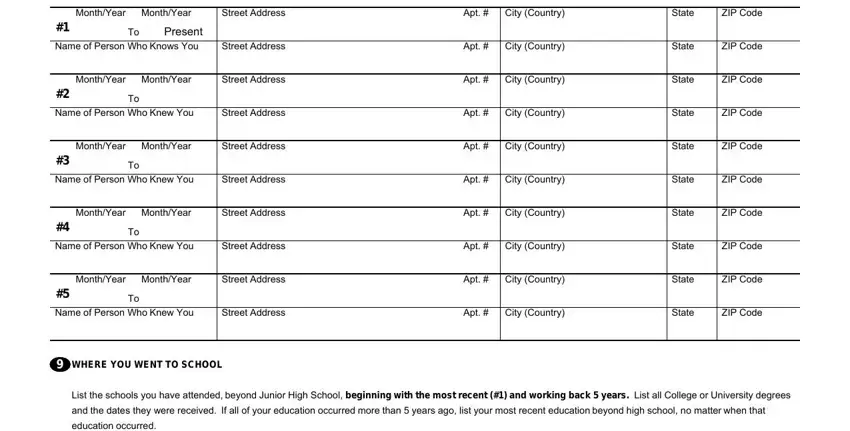
Check the fields MonthYear, MonthYear, Code, Name of School, DegreeDiplomaOther, MonthYear Awarded, Street Address and City Country of, State, ZIP Code, MonthYear, MonthYear, Code, Name of School, DegreeDiplomaOther, and MonthYear Awarded and then fill them out.
Step 3: Click the button "Done". Your PDF form can be transferred. You will be able save it to your computer or email it.
Step 4: Come up with at least a couple of copies of the document to keep clear of any specific possible concerns.
