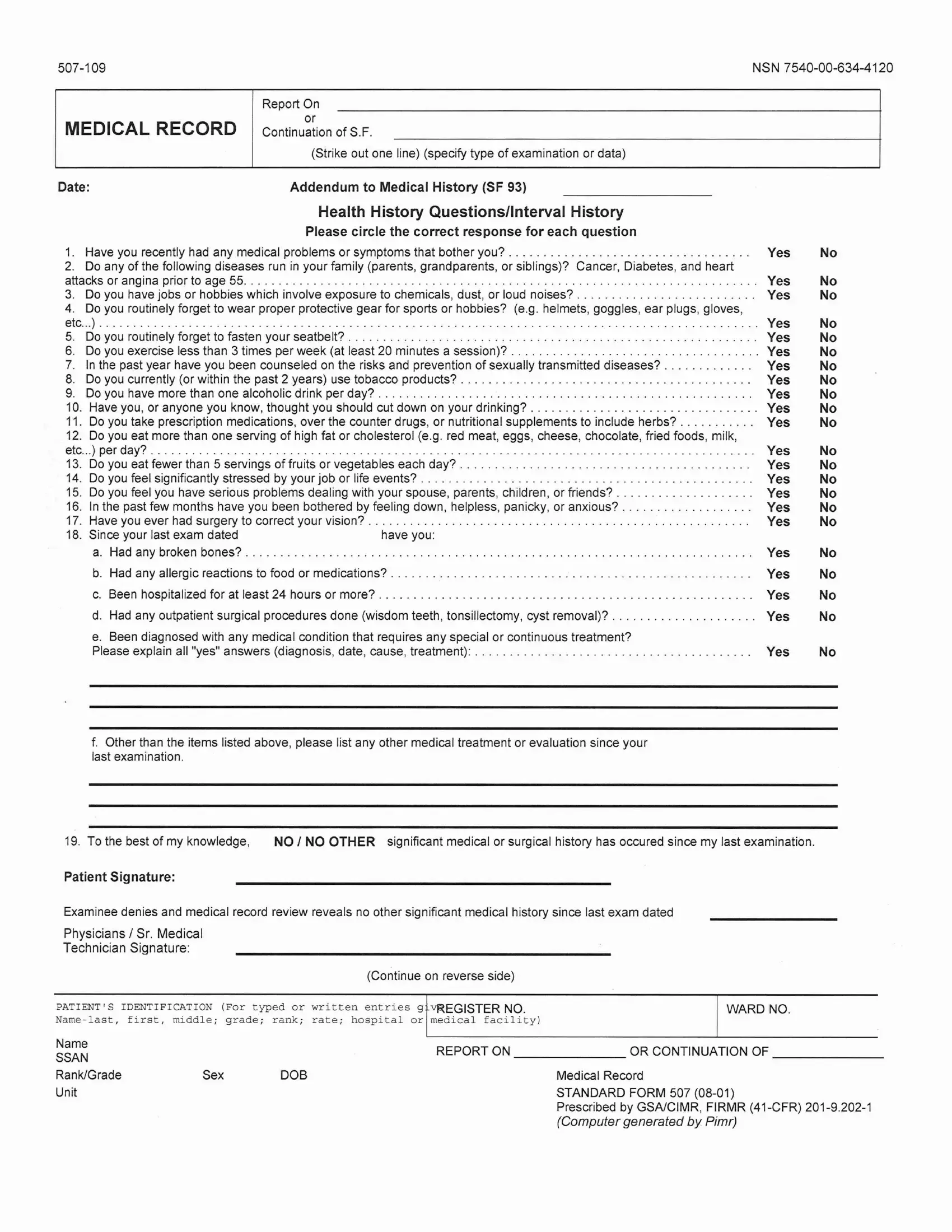
The Standard 507 form serves as a critical tool in the medical field, particularly for comprehensive recording and continuation of medical histories, examination data, and health assessments. It meticulously gathers personal health history, family medical history, lifestyle habits, and potential risk factors that could impact an individual's health status. Specifically designed to augment the Medical History Form (SF 93), the Standard 507 form delves into detailed questions about recent medical issues, genetic diseases prevalent in the family, and behaviors that could predispose individuals to health risks, such as exposure to hazardous materials, neglect in the use of protective gear, unhealthy dietary habits, substance use, and inadequate physical activities. Moreover, it addresses mental health concerns, stressing the significance of acknowledging and addressing symptoms related to stress, depression, anxiety, and relational problems. The process for completing this form is meticulous, requiring truthful and comprehensive responses to each enumerated query, with clear instructions provided for explaining any affirmative answer in detail. This systematic approach ensures that healthcare providers get a well-rounded view of the examinee’s health, guiding them in offering personalized care and preventive measures tailored to the individual's needs and health risks. The form underscores the importance of transparency and accuracy in reporting medical information, thereby facilitating better health outcomes for individuals.
| Question | Answer |
|---|---|
| Form Name | Standard Form 507 |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | form om 501, google army form sf 507, sf 507 blank, online version of word |
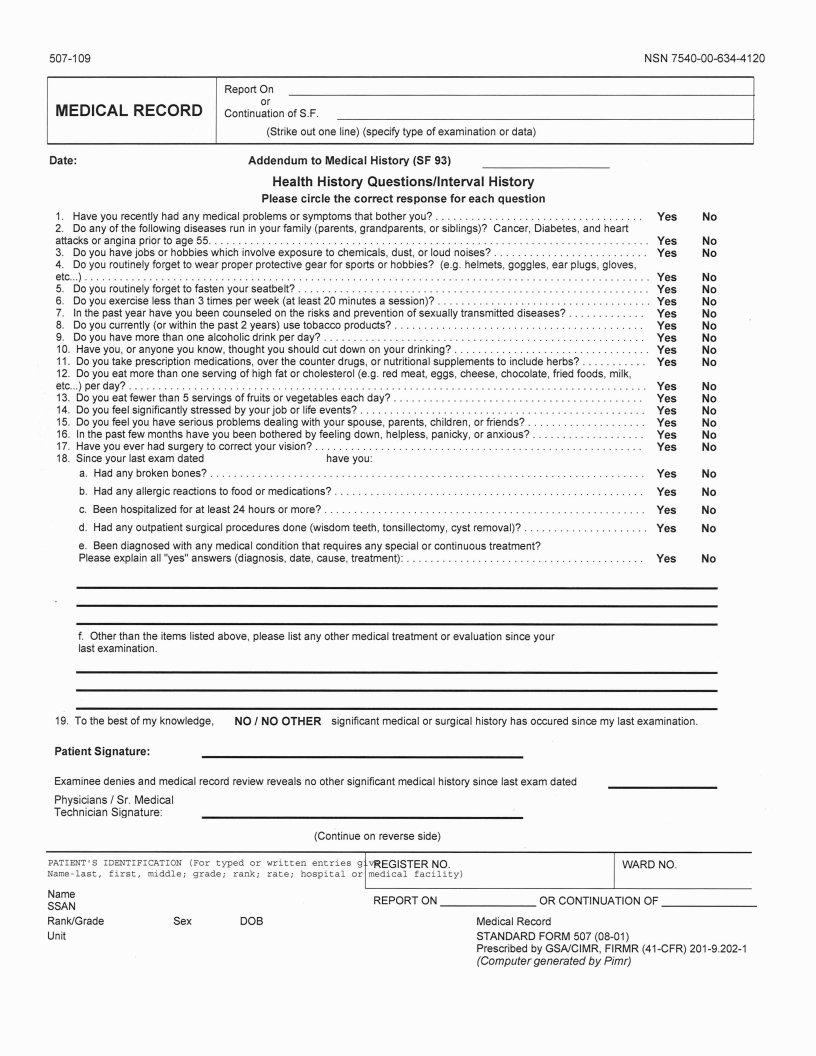
NSN |
Report On
or
MEDICAL RECORD continuation of S.F.
(Strike out one line) (specify type of examination or data)
Date:Addendum to Medical History (SF 93)
Health History Questionsllnterval History
Please circle the correct response for each question
1. |
Have you recently had any medical problems or symptoms that bother you? |
Yes |
No |
|
|
2. Do any of the following diseases run in your family (parents, grandparents, or siblings)? Cancer, Diabetes, and heart |
|
|
|
||
attacksoranginapriortoage55 |
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . |
Yes |
No |
|
|
3. |
Do you have jobs or hobbies which involve exposure to chemicals, dust, or loud noises? |
Yes |
No |
|
|
4. |
Do you routinely forget to wear proper protective gear for sports or hobbies? (e.g. helmets, goggles, ear plugs, gloves, |
|
|
|
|
etc |
.Yes |
No |
|
||
5. |
Do you routinely forget to fasten your seatbelt? |
Yes |
No |
|
|
6. |
Do you exercise less than 3 times per week (at least 20 minutes a session)? |
Yes |
No |
|
|
7. |
In the past year have you been counseled on the risks and prevention of sexually transmitted diseases? |
Yes |
No |
. |
|
8. |
Do you currently (or within the past 2 years) use tobacco products? |
Yes |
No |
|
|
9. |
Do you have more than one alcoholic drink per day? |
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . |
Yes |
No |
|
10. Have you, or anyone you know, thought you should cut down on your drinking? |
Yes |
No |
|
||
11. Do you take prescription medications, over the counter drugs, or nutritional supplements to include herbs? |
Yes |
No |
|
||
12. Do you eat more than one serving of high fat or cholesterol (e.g. red meat, eggs, cheese, chocolate, fried foods, milk, |
|
|
|
||
etc... |
)p erday? |
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . |
Yes |
No |
|
13. Do you eat fewer than 5 servings of fruits or vegetables each day? |
Yes |
No |
|
||
14. Do you feel significantly stressed by your job or life events? |
Yes |
No |
|
||
15. Do you feel you have serious problems dealing with your spouse, parents, children, or friends? |
Yes |
No |
|
||
16. In the past few months have you been bothered by feeling down, helpless, panicky, or anxious? |
Yes |
No |
|
||
17. Have you ever had surgery to correct your vision? |
Yes |
No |
|
||
18. Since your last exam dated |
have you: |
|
|
|
|
|
a. Hadanybrokenbones? |
Yes |
No |
|
|
|
b. Had any allergic reactions to food or medications? |
Yes |
No |
|
|
|
c. Been hospitalizedfor at least 24 hours or more? |
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . |
Yes |
No |
|
|
d. Had any outpatient surgical procedures done (wisdom teeth, tonsillectomy, cyst removal)? |
Yes |
No |
|
|
|
e. Been diagnosed with any medical condition that requires any special or continuous treatment? |
|
|
|
|
|
Please explain all "yes" answers (diagnosis, date, cause, treatment): |
Yes |
No |
|
|
f.Other than the items listed above, please list any other medical treatment or evaluation since your last examination.
19.To the best of my knowledge, NO INO OTHER significant medical or surgical history has occured since my last examination.
Patient Signature:
Examinee denies and medical record review reveals no other significant medical history since last exam dated
Physicians / Sr. Medical
Technician Signature:
(continue on reverse side)
PATIENT'S IDENTIFICATION (For typed or written entries g qEGISTER NO. |
WARD NO. |
|||
|
||||
Name |
|
REPORT ON |
OR CONTINUATION OF |
|
SSAN |
|
|||
|
|
|
||
Rank1Grade |
Sex |
DOB |
Medical Record |
|
Unit |
|
|
STANDARD FORM 507 |
|
|
|
|
Prescribed by GSAICIMR, FlRMR |
|
|
|
|
(Computer generated by Pimr) |
|
Procedures for Completing the SF507
PLEASE READ, DO NOT ANSWER ON THIS FORM
Dear 157th ARW Member,
Since the implementation of the PHA process and SF 507 we have noticed that required medical information has been left off the SF 507. In an effort to ensure that the SF 507 is completed accurately and with the appropriate information, we have developed this form to help you complete the SF 507. Please use it as you complete your SF 507. If you have any questions or concerns regarding this matter, please feel free to contact the Medical Group at X2340. Thank you for your help and cooperation
1.When you answer with a positive response (yes) to any question on the SF507 you are required to supply the appropriate information listed in the action section for each question.
2.Please explain all positive response (yes) answers on the back of the SF507, by placing the question number in front of each explanation.
|
|
QUESTION |
IF YES: |
ACTION |
|
|
|
|
|
|
|
|
1 |
Have you recently had any medical problem or symptoms that bother |
State medical problem and symptoms. |
|
|
|
|
you? |
|
|
|
|
|
|
|
|
|
|
2 |
Do any of the following diseases run in your family? Cancer, |
List the disease and state the relationship of |
|
|
|
|
Diabetes, and heart attacks or angina prior to age 55. |
the person who has the disease to you. |
|
|
|
|
|
|
|
|
|
3 |
Do you have job or hobbies, which involve exposure to chemicals, |
List the job/hobbies also list what you are |
|
|
|
|
dust, or loud noise? |
exposed to. |
|
|
|
|
|
|
|
|
|
4 |
Do you routinely forget to wear proper protective gear for sports or |
List the names of sports/ hobbies. |
|
|
|
|
hobbies? |
|
|
|
|
|
|
|
|
|
|
5 |
Do you routinely forget to fasten your seatbelt? |
Yes or No answer |
|
|
|
|
|
|
|
|
|
6 |
Do you exercise less than 3 times per week? ( at least 20 minutes a |
Yes or No answer |
|
|
|
|
session) |
|
|
|
|
|
|
|
|
|
|
7 |
In the past year have you been counseled on the risks and |
State if counseling was a preventive health/ |
|
|
|
|
prevention of sexually transmitted diseases? |
|
||
|
|
|
treatment. |
|
|
|
8 |
Do you currently (or within the past 2 years) use tobacco products? |
State the type of tobacco product you use; the |
|
|
|
|
|
amount per day you use, and how long you |
|
|
|
|
|
have been using. |
|
|
|
|
|
|
|
|
|
9 |
Do you have more than one alcoholic drink per day? |
State how many alcoholic drinks you consume |
|
|
|
|
|
per day. |
|
|
|
|
|
|
|
|
|
10 |
Have you, or anyone you now, thought you should cut down on your |
Briefly explain. |
|
|
|
|
drinking? |
|
|
|
|
|
|
|
|
|
|
11 |
Do you take prescription medication, over the counter drugs or |
List the name of the medication/supplement |
|
|
|
|
nutritional supplements to include herbs? |
and what it is taken for. Give the amount taken |
|
|
|
|
|
and how often taken. |
|
|
|
|
|
|
|
|
|
12 |
Do you eat more than one serving of high fat or cholesterol per day? |
Yes or No answer. |
|
|
|
|
|
|
|
|
|
13 |
Do you eat fewer than 5 servings of fruits or vegetables each day? |
Yes or No answer. |
|
|
|
|
|
|
|
|
|
14 |
Do you feel you have a high stress job or life style? |
Briefly explain. |
|
|
|
|
|
|
|
|
|
15 |
Do you feel you have serious problems dealing with your spouse, |
Briefly explain. |
|
|
|
|
parents, children or friends? |
|
|
|
|
|
|
|
|
|
|
16 |
In the past few months have you been bothered by feeling down, |
Briefly explain. |
|
|
|
|
helpless, panicky, or anxious? |
|
|
|
|
|
|
|
|
|
|
17 |
Have you ever had surgery to correct your vision? |
State when and where surgery was done. |
|
|
|
|
|
|
|
|
|
18 |
Since your last exam have you? |
a. List bone broken and when |
|
|
|
|
|
b. List allergy and reaction |
|
|
|
|
|
c. List reason for hospitalization and when |
|
|
|
|
|
d. list procedure and when. |
|
|
|
|
|
e. List new medical condition and treatment. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|