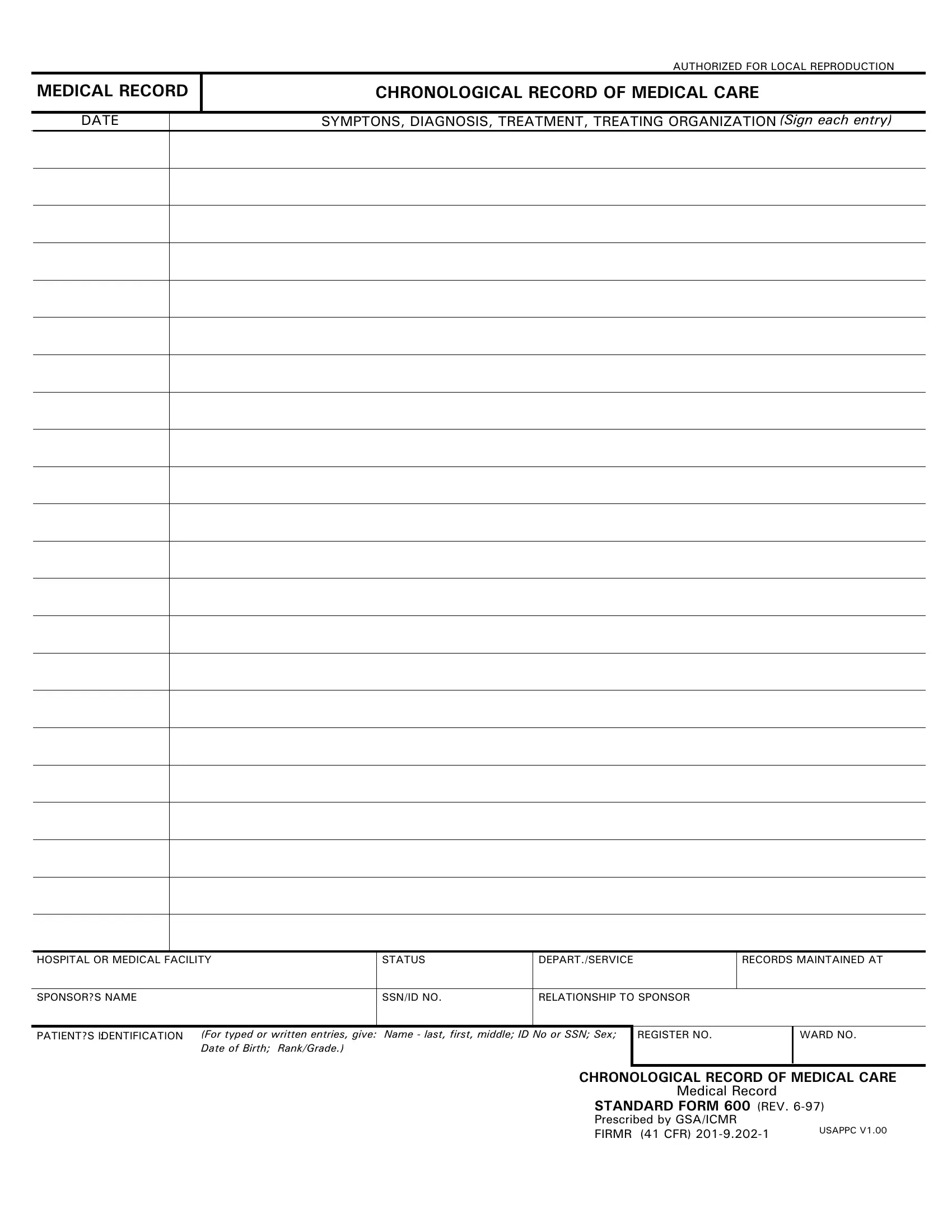
The Standard Form 600 (SF 600) serves a critical function within the landscape of medical documentation, enabling a detailed and chronological record of medical care to be meticulously maintained. By design, this form facilitates the systematic capture of a patient's medical interactions, ranging from symptoms and diagnoses to treatments administered by specific organizations, whether in hospitals or other medical facilities. The importance of such detailed record-keeping cannot be understated, as it ensures continuity of care, supports accurate medical evaluation, and enhances the overall management of patient health outcomes. Elements such as the patient's identification details, including but not limited to name, social security number (SSN) or identification number (ID), sex, date of birth, and rank or grade, are systematically recorded alongside the clinical narrative detailing each medical event. The form's structure also makes provisions for noting the status of the patient within the medical or hospital framework, the department or service maintaining the records, as well as the patient's sponsor information. The SF 600’s comprehensive nature and its authorization for local reproduction underlines its value and utility across various facets of healthcare documentation, governed by standards set by the General Services Administration (GSA) and the Interagency Committee on Medical Records (ICMR), showcasing its pivotal role in ensuring meticulous and consistent medical record-keeping.
| Question | Answer |
|---|---|
| Form Name | SF 600 Form |
| Form Length | 1 pages |
| Fillable? | Yes |
| Fillable fields | 53 |
| Avg. time to fill out | 10 min 51 sec |
| Other names | s600 sf600 form |
AUTHORIZED FOR LOCAL REPRODUCTION
MEDICAL RECORD
CHRONOLOGICAL RECORD OF MEDICAL CARE
DATE
SYMPTONS, DIAGNOSIS, TREATMENT, TREATING ORGANIZATION (Sign each entry)
HOSPITAL OR MEDICAL FACILITY
STATUS
DEPART./SERVICE
RECORDS MAINTAINED AT
SPONSOR?S NAME
SSN/ID NO.
RELATIONSHIP TO SPONSOR
PATIENT?S IDENTIFICATION: |
(For typed or written entries, give: Name - last, first, middle; ID No or SSN; Sex; |
|
Date of Birth; Rank/Grade.) |
REGISTER NO.
WARD NO.
CHRONOLOGICAL RECORD OF MEDICAL CARE
Medical Record
STANDARD FORM 600 (REV.
Prescribed by GSA/ICMR
FIRMR (41 CFR) |
USAPPC V1.00 |
|