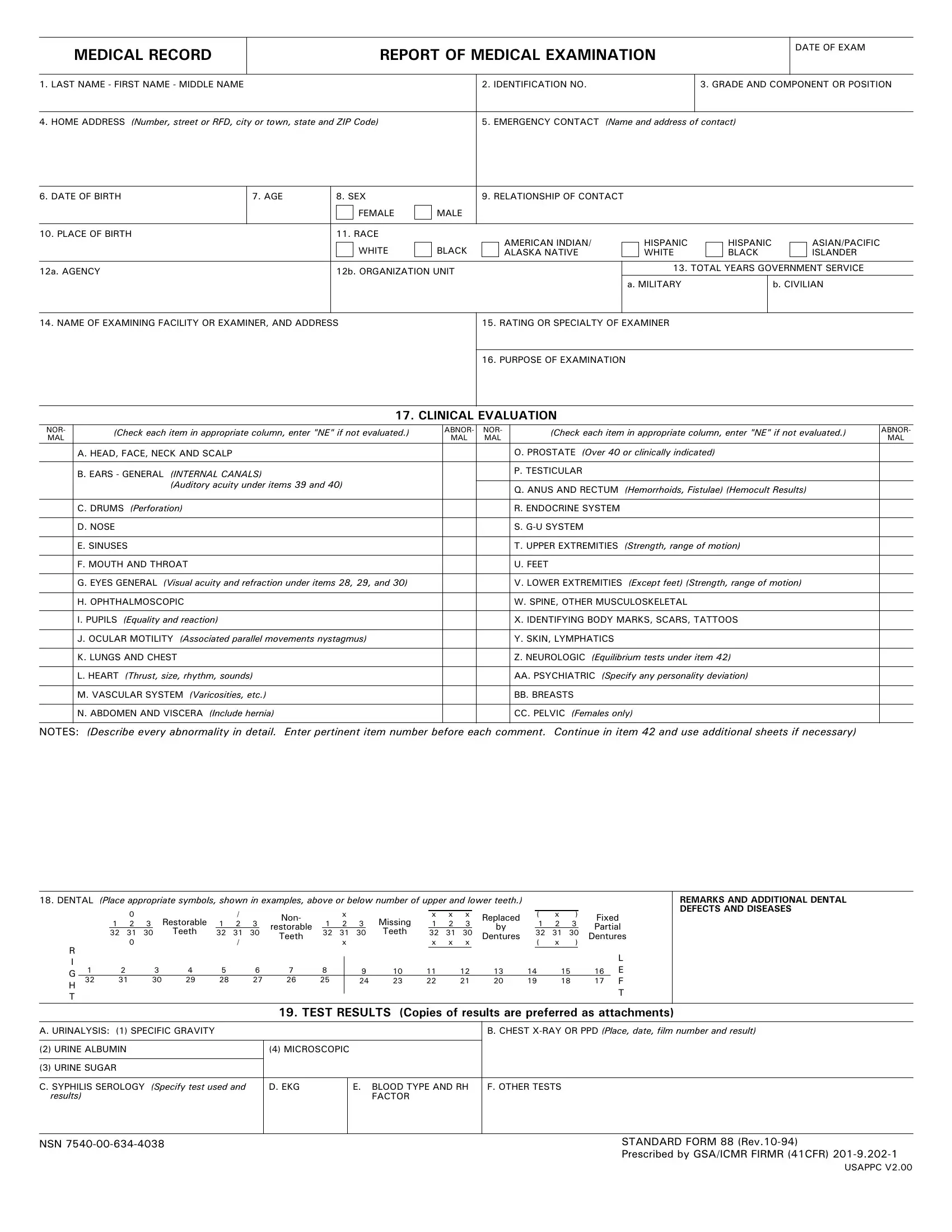
When it comes to comprehensive health assessments, the Standard Form 88 (SF-88), known as the "Report of Medical Examination," is a critical document commonly used in various federal employment and military settings. This detailed form captures a wide array of personal and health-related information, ranging from basic identifiers like name and date of birth to intricate details regarding an individual's medical examination results. The form meticulously outlines components such as emergency contact information, identification numbers, and demographic specifics, including race and place of birth. Additionally, the SF-88 delves into the clinical evaluation of numerous health aspects, such as vision and hearing acuity, the condition of the heart, lungs, and vascular system, psychological and psychiatric assessments, and even dental health. Moreover, it incorporates results from various tests including urinalysis, chest X-rays, blood typing, and more. Such thorough medical documentation serves multiple purposes, from assessing fitness for duty to identifying potential health problems, thereby playing a crucial role in managing the well-being of government employees and military personnel.
| Question | Answer |
|---|---|
| Form Name | Standard Form 88 |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | standard form 88 army fillable, sf 88 and sf 93, sf88, sf88 form |
MEDICAL RECORD
REPORT OF MEDICAL EXAMINATION
DATE OF EXAM
1. LAST NAME - FIRST NAME - MIDDLE NAME |
2. IDENTIFICATION NO. |
3. GRADE AND COMPONENT OR POSITION |
|
|
|
4. HOME ADDRESS (Number, street or RFD, city or town, state and ZIP Code) |
5. EMERGENCY CONTACT (Name and address of contact) |
|
6. DATE OF BIRTH |
7. AGE |
|
8. SEX |
|
|
|
9. RELATIONSHIP OF CONTACT |
|
|
|
|
|
|
|
|
|||
|
|
|
|
FEMALE |
|
MALE |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
10. PLACE OF BIRTH |
|
|
11. RACE |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
WHITE |
|
BLACK |
|
|
AMERICAN INDIAN/ |
|
|
HISPANIC |
|
HISPANIC |
|
|
ASIAN/PACIFIC |
|
|
|
|
|
|
|
|
ALASKA NATIVE |
|
|
WHITE |
|
BLACK |
|
|
ISLANDER |
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
12a. AGENCY |
|
|
12b. ORGANIZATION UNIT |
|
|
|
|
|
13. TOTAL YEARS GOVERNMENT SERVICE |
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
a. MILITARY |
|
|
b. CIVILIAN |
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
14. NAME OF EXAMINING FACILITY OR EXAMINER, AND ADDRESS |
|
|
|
15. RATING OR SPECIALTY OF EXAMINER |
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
16. PURPOSE OF EXAMINATION |
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
17. CLINICAL EVALUATION
NOR- |
(Check each item in appropriate column, enter "NE" if not evaluated.) |
ABNOR- |
NOR- |
(Check each item in appropriate column, enter "NE" if not evaluated.) |
ABNOR- |
||
MAL |
MAL |
MAL |
MAL |
||||
|
|
|
|||||
|
A. HEAD, FACE, NECK AND SCALP |
|
|
O. PROSTATE (Over 40 or clinically indicated) |
|
||
|
|
|
|
|
|
|
|
|
B. EARS - GENERAL (INTERNAL CANALS) |
|
|
P. TESTICULAR |
|
|
|
|
|
|
|
|
|
||
|
(Auditory acuity under items 39 and 40) |
|
|
Q. ANUS AND RECTUM (Hemorrhoids, Fistulae) (Hemocult Results) |
|
||
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
C. DRUMS (Perforation) |
|
|
R. ENDOCRINE SYSTEM |
|
|
|
|
|
|
|
|
|
|
|
|
D. NOSE |
|
|
S. |
|
|
|
|
|
|
|
|
|
|
|
|
E. SINUSES |
|
|
T. UPPER EXTREMITIES |
(Strength, range of motion) |
|
|
|
|
|
|
|
|
|
|
|
F. MOUTH AND THROAT |
|
|
U. FEET |
|
|
|
|
|
|
|
|
|
||
|
G. EYES GENERAL (Visual acuity and refraction under items 28, 29, and 30) |
|
|
V. LOWER EXTREMITIES (Except feet) (Strength, range of motion) |
|
||
|
|
|
|
|
|
||
|
H. OPHTHALMOSCOPIC |
|
|
W. SPINE, OTHER MUSCULOSKELETAL |
|
||
|
|
|
|
|
|
||
|
I. PUPILS (Equality and reaction) |
|
|
X. IDENTIFYING BODY MARKS, SCARS, TATTOOS |
|
||
|
|
|
|
|
|
|
|
|
J. OCULAR MOTILITY (Associated parallel movements nystagmus) |
|
|
Y. SKIN, LYMPHATICS |
|
|
|
|
|
|
|
|
|
||
|
K. LUNGS AND CHEST |
|
|
Z. NEUROLOGIC (Equilibrium tests under item 42) |
|
||
|
|
|
|
|
|
||
|
L. HEART (Thrust, size, rhythm, sounds) |
|
|
AA. PSYCHIATRIC (Specify any personality deviation) |
|
||
|
|
|
|
|
|
|
|
|
M. VASCULAR SYSTEM (Varicosities, etc.) |
|
|
BB. BREASTS |
|
|
|
|
|
|
|
|
|
||
|
N. ABDOMEN AND VISCERA (Include hernia) |
|
|
CC. PELVIC (Females only) |
|
||
|
|
|
|
|
|
|
|
NOTES: (Describe every abnormality in detail. Enter pertinent item number before each comment. Continue in item 42 and use additional sheets if necessary)
18.DENTAL (Place appropriate symbols, shown in examples, above or below number of upper and lower teeth.)
|
|
|
0 |
|
|
Restorable |
|
/ |
|
|
Non- |
|
|
x |
|
|
Missing |
|
x |
x |
x |
|
Replaced |
|
( |
x |
) |
Fixed |
||
|
|
1 |
2 |
3 |
|
1 |
2 |
3 |
|
restorable |
|
1 |
2 |
3 |
|
|
1 |
2 |
3 |
|
by |
|
1 |
2 |
3 |
Partial |
||||
|
32 31 |
30 |
Teeth |
32 |
31 |
30 |
32 |
31 |
30 |
Teeth |
32 |
31 |
30 |
32 |
31 |
30 |
||||||||||||||
|
Teeth |
Dentures |
Dentures |
|||||||||||||||||||||||||||
|
|
|
0 |
|
|
|
|
/ |
|
|
|
|
|
x |
|
|
|
|
x |
x |
x |
|
( |
x |
) |
|
|
|||
R |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
L |
I |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
E |
|
G |
1 |
|
2 |
3 |
4 |
5 |
|
6 |
7 |
8 |
|
|
9 |
10 |
11 |
|
12 |
|
13 |
14 |
15 |
16 |
||||||||
32 |
|
31 |
30 |
29 |
28 |
|
27 |
26 |
25 |
|
|
24 |
23 |
22 |
|
21 |
|
20 |
19 |
18 |
17 |
F |
||||||||
H |
|
|
|
|
|
|
||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
T |
|
T |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
REMARKS AND ADDITIONAL DENTAL DEFECTS AND DISEASES
19. TEST RESULTS (Copies of results are preferred as attachments)
A. URINALYSIS: (1) SPECIFIC GRAVITY |
|
|
|
|
B. CHEST |
|
|
|
|
|
|
(2) URINE ALBUMIN |
(4) MICROSCOPIC |
|
|
|
|
|
|
|
|
|
|
(3) URINE SUGAR |
|
|
|
|
|
|
|
|
|
||
C. SYPHILIS SEROLOGY (Specify test used and |
D. EKG |
|
E. BLOOD TYPE AND RH |
F. OTHER TESTS |
|
results) |
|
|
FACTOR |
|
|
|
|
|
|
|
|
NSN |
STANDARD FORM 88 |
|
|
|
Prescribed by GSA/ICMR FIRMR (41CFR) |
USAPPC V2.00
NAME
IDENTIFICATION NUMBER
NO. OF SHEETS ATTACHED
MEASUREMENTS AND OTHER FINDINGS
20. HEIGHT
21. WEIGHT
22. COLOR HAIR
23. COLOR EYES
24. BUILD:
SLENDER
MEDIUM
HEAVY
OBESE
25. TEMPERATURE
|
|
26. BLOOD PRESSURE (Arm at heart level) |
|
|
|
|
|
27. PULSE (Arm at heart level) |
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
A. |
SYS. |
|
B. |
SYS. |
C. |
SYS. |
|
A. SITTING |
|
B. RECUMBENT |
C. STANDING |
D. AFTER EXERCISE |
E. 2 MINS. AFTER |
|
|
|
|
||||||||||
|
|
|
RECUM- |
|
|
|
|
|
|
|
(3 MINS) |
|
|
SITTING |
DIAS. |
|
DIAS. |
STANDING |
DIAS. |
|
|
|
|
|
|
|
|
|
BENT |
|
|
|
|
|
|
|
|||||
|
|
|
|
|
(5 mins.) |
|
|
|
|
|
|
|
|
|
28. DISTANT VISION |
|
|
|
29. REFRACTION |
|
|
|
30. NEAR VISION |
||||
|
|
|
|
|
|
|
|
|
|
|
|||
RIGHT 20/ |
|
CORR. TO 20/ |
|
BY |
|
S. |
CX |
|
CORR. TO |
BY |
|||
|
|
|
|
|
|
|
|
|
|
|
|||
LEFT 20/ |
|
CORR. TO 20/ |
|
BY |
|
S. |
CX |
|
CORR. TO |
BY |
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
31.HETEROPHORIA (Specify distance)
ESO |
EXO |
R.H. |
|
|
L.H. |
|
|
PRISM DIV. |
|
|
PRISM CONV. |
PC |
PD |
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
CT |
|
|
|
32. ACCOMMODATION |
|
|
33. COLOR VISION (Test used and result) |
|
|
|
|
34. DEPTH PERCEPTION |
|
UNCORRECTED |
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
(Test used and score) |
|
|
|
RIGHT |
LEFT |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
CORRECTED |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
35. FIELD OF VISION |
|
|
36. NIGHT VISION (Test used and score) |
|
|
|
|
37. RED LENS TEST |
|
38. INTRAOCULAR TENSION |
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
RIGHT |
LEFT |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
RIGHT |
LEFT |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
39. HEARING |
|
|
|
|
|
40. AUDIOMETER |
|
|
|
|
41. PSYCHOLOGICAL AND PSYCHOMOTOR (Tests used and scores) |
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
RIGHT WV |
/15 SV |
/15 |
|
|
250 |
500 |
1000 |
2000 |
3000 |
4000 |
6000 |
8000 |
|
|
|
|
|
|
|
256 |
512 |
1024 |
2048 |
2896 |
4096 |
6144 |
8192 |
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
RIGHT |
|
|
|
|
|
|
|
|
|
|
|
|
|
LEFT WV |
/15 SV |
/15 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
LEFT |
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
42. NOTES (Continued) |
AND SIGNIFICANT OR INTERVAL HISTORY |
|
|
|
|
|
|
|
|
|
|
|
|
||||
(Use additional sheets if necessary)
43.SUMMARY OF DEFECTS AND DIAGNOSES (List diagnoses with item numbers)
44. |
RECOMMENDATIONS - FURTHER SPECIALIST EXAMINATIONS INDICATED (Specify) |
|
|
|
|
45A. PHYSICAL PROFILE |
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
P |
|
U |
L |
|
H |
E |
|
S |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
46. |
EXAMINEE (Check) |
|
|
|
|
|
|
|
|
|
|
||
A. |
|
IS QUALIFIED FOR |
|
|
|
|
45B. PHYSICAL CATEGORY |
|
|||||
|
|
|
|
|
|
||||||||
B. |
|
IS NOT QUALIFIED FOR |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|||
47. |
IF NOT QUALIFIED, LIST DISQUALIFYING DEFECTS BY ITEM NUMBER |
|
A |
|
B |
|
|
C |
|
E |
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
48. TYPED OR PRINTED NAME OF PHYSICIAN
SIGNATURE
49. TYPED OR PRINTED NAME OF PHYSICIAN
SIGNATURE
50. TYPED OR PRINTED NAME OF DENTIST OR PHYSICIAN (Indicate which)
SIGNATURE
51. TYPED OR PRINTED NAME OF REVIEWING OFFICER OR APPROVING AUTHORITY
SIGNATURE
STANDARD FORM 88 (Rev.
USAPPC V2.00