
Should you intend to fill out Verifier, you don't have to install any applications - just give a try to our online tool. To maintain our editor on the leading edge of practicality, we work to put into action user-oriented features and enhancements on a regular basis. We're routinely pleased to get suggestions - assist us with reshaping how we work with PDF documents. Here's what you would want to do to get going:
Step 1: Open the PDF in our editor by clicking the "Get Form Button" in the top section of this webpage.
Step 2: Once you open the online editor, you will notice the form prepared to be filled in. Aside from filling out various blanks, you might also do several other things with the form, such as putting on your own text, modifying the initial textual content, adding graphics, placing your signature to the form, and much more.
Completing this PDF will require thoroughness. Ensure that every single blank is filled in properly.
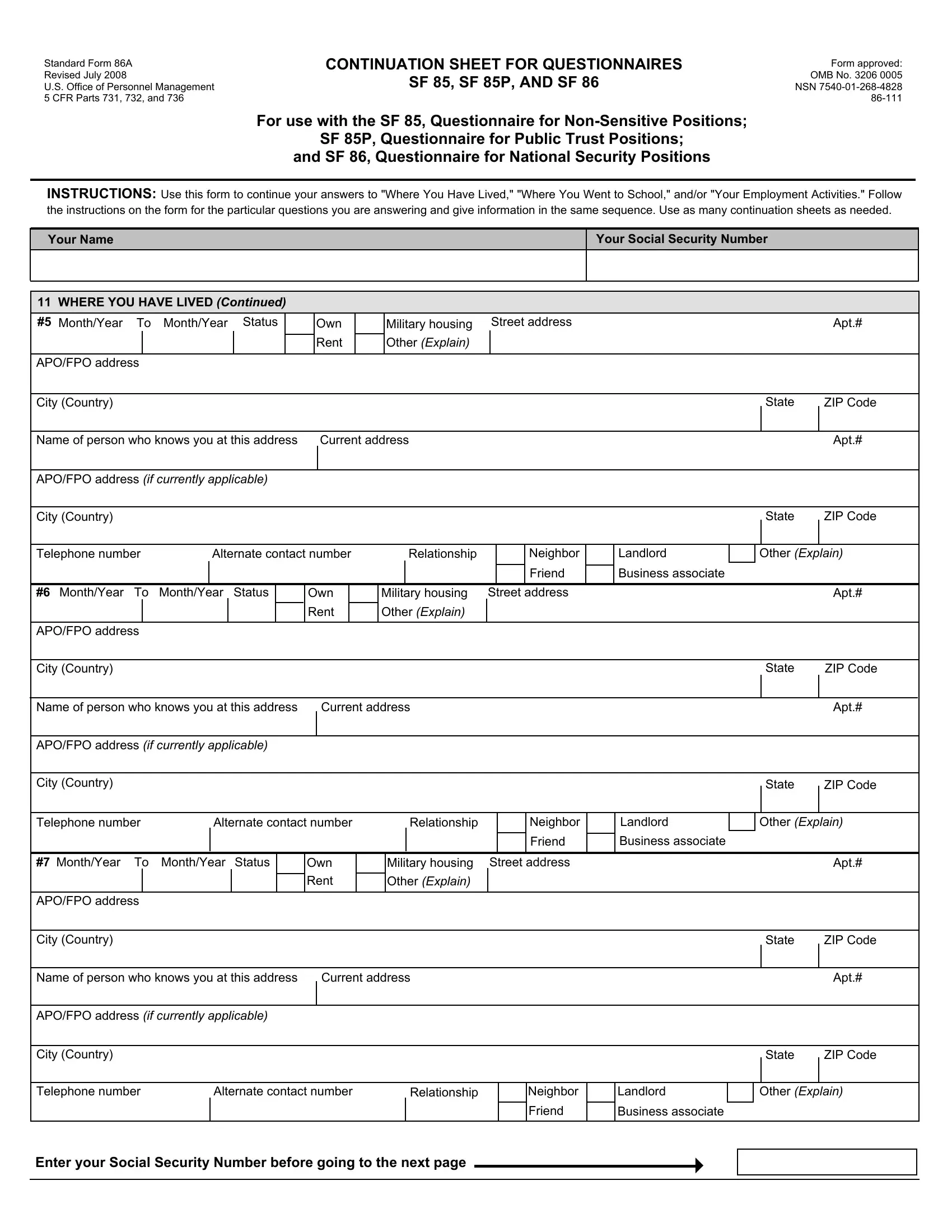
1. While filling in the Verifier, make sure to incorporate all of the essential blanks within the relevant form section. It will help expedite the process, which allows your details to be processed promptly and correctly.
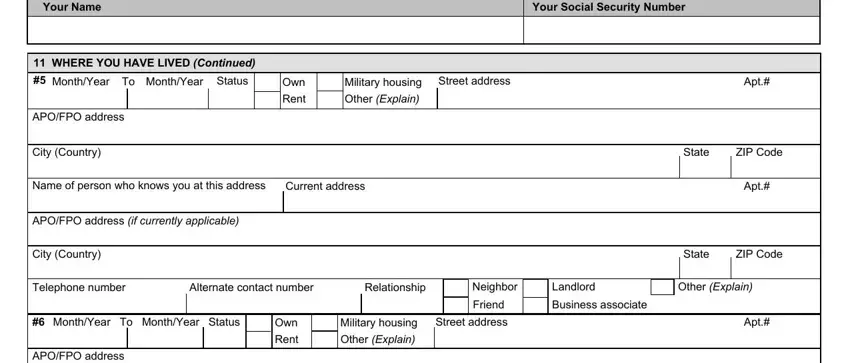
2. Just after completing the previous section, head on to the subsequent part and enter all required particulars in all these blank fields - City Country, Name of person who knows you at, Current address, APOFPO address if currently, City Country, State, ZIP Code, Apt, State, ZIP Code, Telephone number, Alternate contact number, Relationship, Neighbor, and Landlord.
Concerning ZIP Code and Relationship, be sure that you double-check them in this current part. Those two are the most important fields in this form.
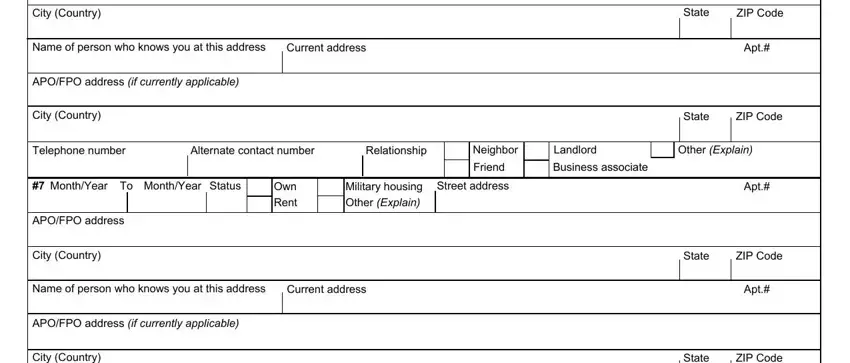
3. The following portion is all about City Country, State, ZIP Code, Telephone number, Alternate contact number, Relationship, Neighbor, Landlord, Other Explain, Friend, Business associate, and Enter your Social Security Number - complete each of these blank fields.

4. You're ready to proceed to the next segment! Here you'll get all these WHERE YOU WENT TO SCHOOL Continued, MonthYear, MonthYear, Code, Name of school, Street address and City Country of, Name of person who knows you, Current address, Degreediploma received If Yes, State, ZIP Code, Apt, City Country, State, and ZIP Code blanks to fill in.
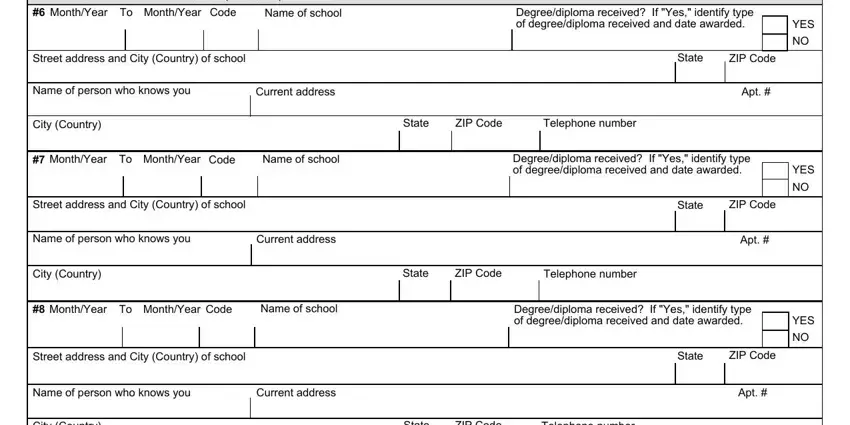
5. Now, this final part is what you need to finish before submitting the form. The blanks at issue are the following: City Country, State, ZIP Code, Telephone number, MonthYear, MonthYear, Code, Name of school, Degreediploma received If Yes, Street address and City Country of, Name of person who knows you, Current address, State, ZIP Code, and Apt.
Step 3: Soon after proofreading your fields and details, press "Done" and you are done and dusted! Find the Verifier as soon as you sign up for a 7-day free trial. Readily gain access to the pdf document inside your FormsPal account page, together with any modifications and changes being automatically saved! At FormsPal, we do our utmost to guarantee that all of your information is maintained private.