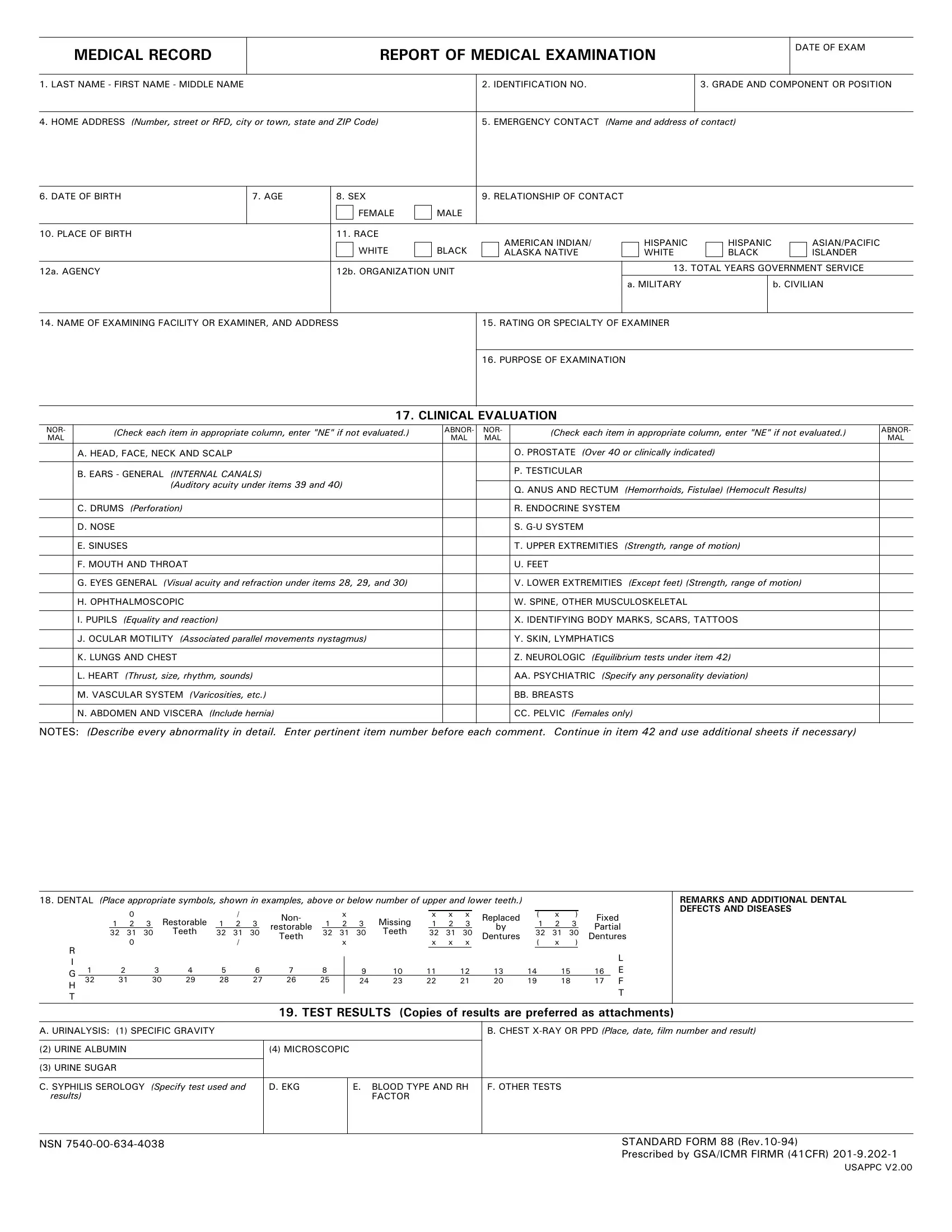
When it comes to comprehensive health assessments, the Standard Form 88 (SF-88), known as the "Report of Medical Examination," is a critical document commonly used in various federal employment and military settings. This detailed form captures a wide array of personal and health-related information, ranging from basic identifiers like name and date of birth to intricate details regarding an individual's medical examination results. The form meticulously outlines components such as emergency contact information, identification numbers, and demographic specifics, including race and place of birth. Additionally, the SF-88 delves into the clinical evaluation of numerous health aspects, such as vision and hearing acuity, the condition of the heart, lungs, and vascular system, psychological and psychiatric assessments, and even dental health. Moreover, it incorporates results from various tests including urinalysis, chest X-rays, blood typing, and more. Such thorough medical documentation serves multiple purposes, from assessing fitness for duty to identifying potential health problems, thereby playing a crucial role in managing the well-being of government employees and military personnel.
| Question | Answer |
|---|---|
| Form Name | Standard Form 88 |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | standard form 88 army fillable, sf 88 and sf 93, sf88, sf88 form |
