

In case you desire to fill out false, it's not necessary to install any sort of software - simply try our PDF tool. The editor is constantly maintained by our staff, acquiring handy features and growing to be much more convenient. To get the process started, take these basic steps:
Step 1: Hit the "Get Form" button above. It is going to open up our pdf editor so you could start filling in your form.
Step 2: With this state-of-the-art PDF tool, it's possible to do more than simply complete blank form fields. Express yourself and make your docs seem faultless with customized textual content added in, or modify the file's original input to perfection - all that accompanied by the capability to insert almost any images and sign the PDF off.
Pay attention while filling in this document. Ensure that all mandatory blanks are filled out properly.
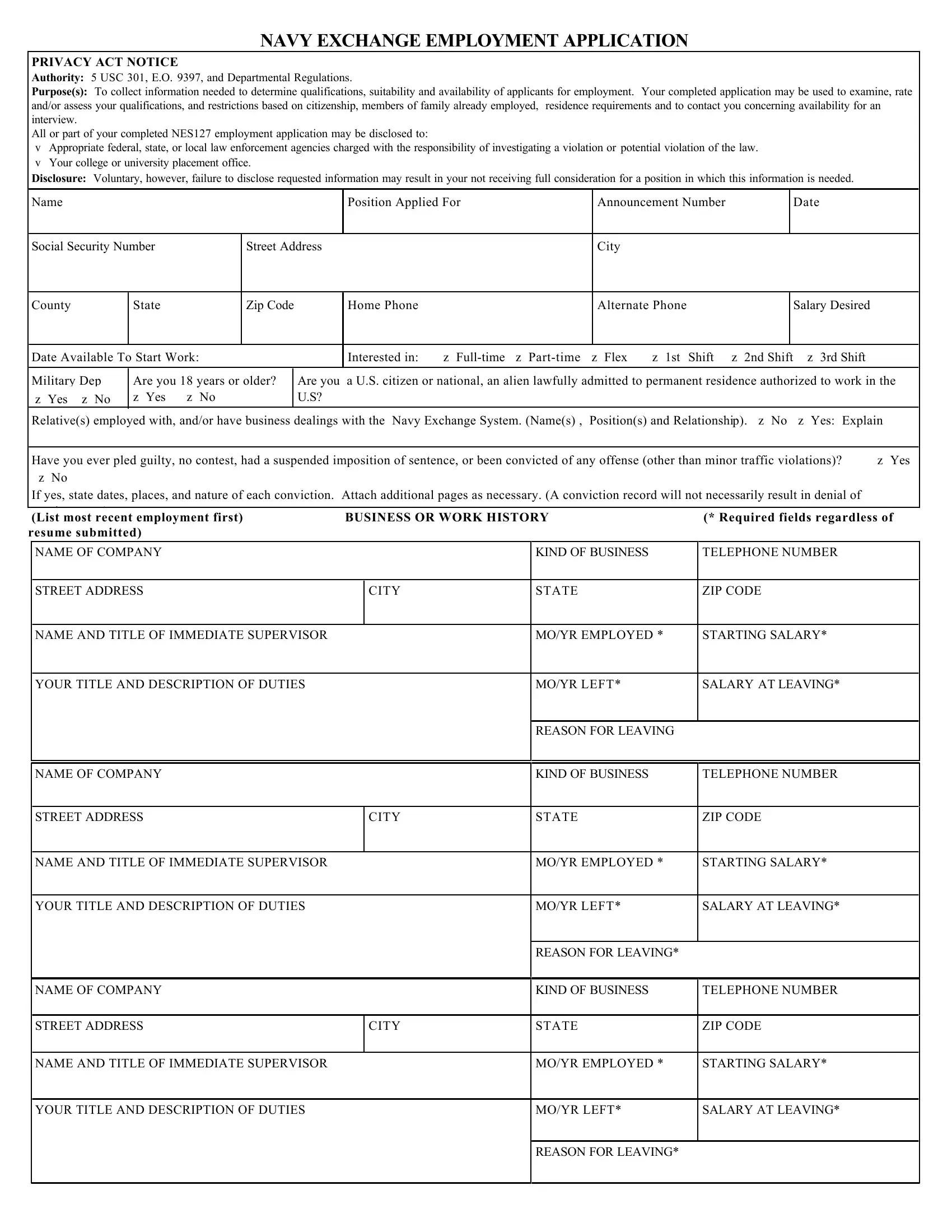
1. First of all, once filling in the false, start in the area that features the following blanks:
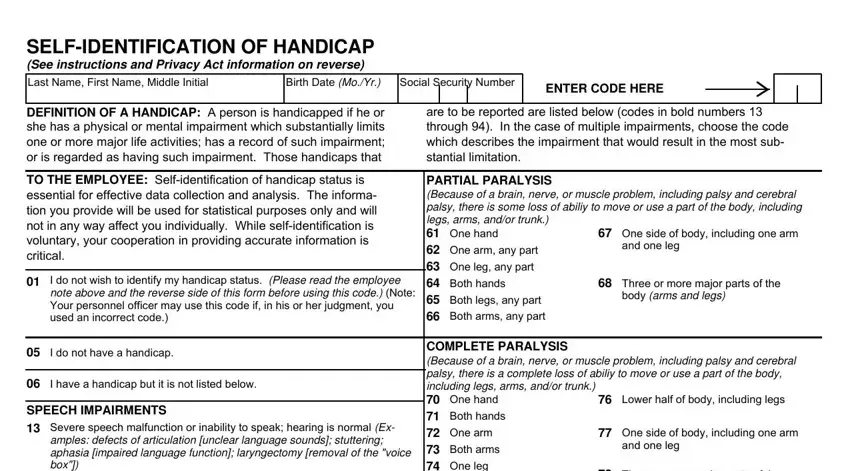
2. Your next part is usually to fill in these particular blank fields: Previous edition unusable, and Standard Form Rev US Office of.

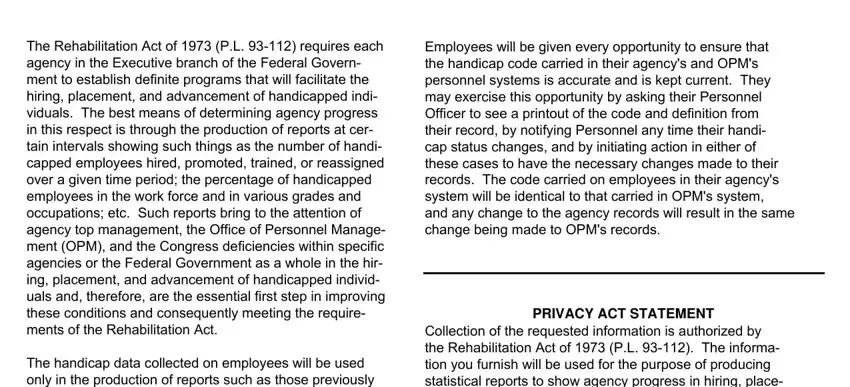
3. Your next step is generally simple - fill out all the blanks in The Rehabilitation Act of PL, The handicap data collected on, Employees will be given every, PRIVACY ACT STATEMENT, and Collection of the requested in order to finish this part.
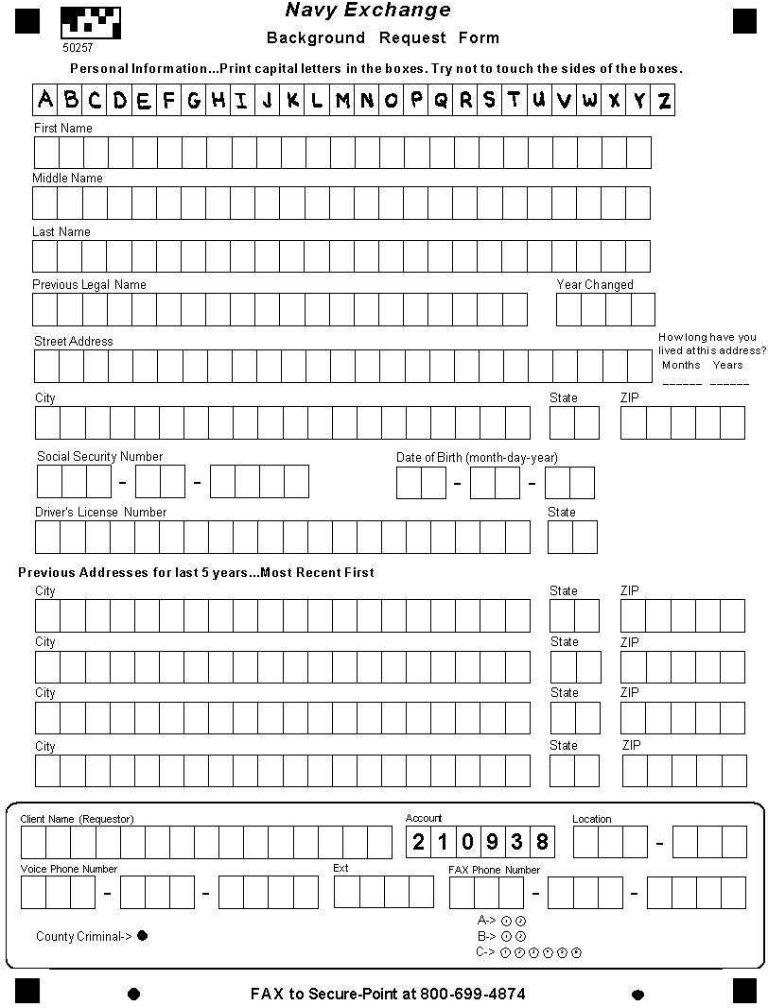
4. It's time to fill out this fourth portion! Here you will get all of these Standard Form BACK, and US GPO blank fields to fill out.

Lots of people often get some things wrong while filling out Standard Form BACK in this area. You should reread whatever you enter here.
Step 3: Confirm that the information is right and simply click "Done" to complete the project. Acquire the false the instant you subscribe to a 7-day free trial. Instantly view the document within your FormsPal account page, with any modifications and changes being conveniently synced! With FormsPal, you'll be able to fill out documents without being concerned about information incidents or entries getting distributed. Our protected software helps to ensure that your personal details are kept safely.