The whole process of filling out the 2013 is really quick. Our team made certain our editor is not hard to utilize and can help fill in virtually any form in no time. Listed here are the four simple steps you need to follow:
Step 1: Pick the button "Get Form Here".
Step 2: Now, you're on the document editing page. You can add information, edit current information, highlight particular words or phrases, place crosses or checks, add images, sign the template, erase unwanted fields, etc.
Enter the required information in every single segment to complete the PDF 2013
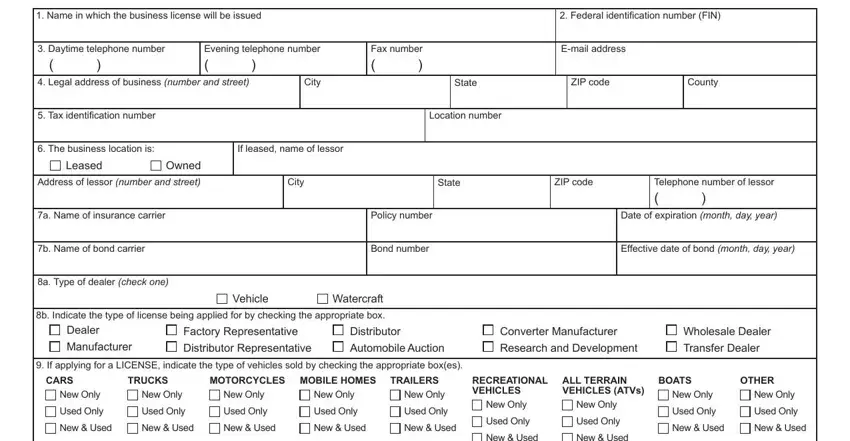
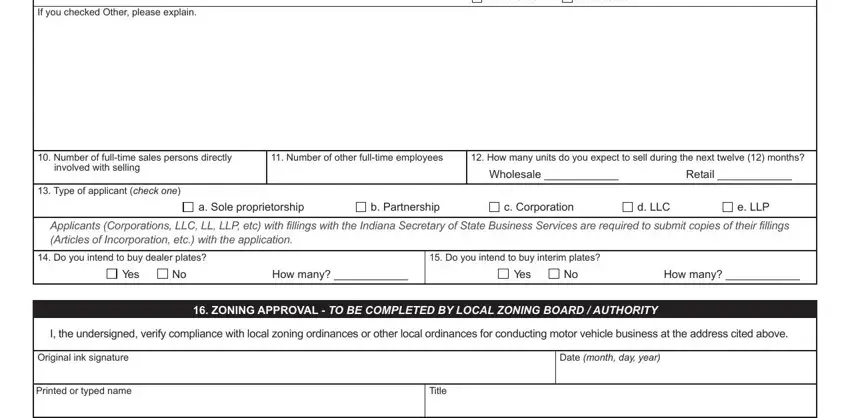
Inside the field If you checked Other please explain, New Used, New Used, Number of fulltime sales persons, involved with selling, Type of applicant check one, Number of other fulltime employees, How many units do you expect to, Wholesale, Retail, a Sole proprietorship, b Partnership, c Corporation, d LLC, and e LLP note the data that the program requests you to do.
Highlight the key details of the Authorizing agency, and Page of part.

The OWNER OFFICER INFORMATION, A Name of primary owner, Home address number and street, City, B Name of additional owner, Home address number and street, City, C Name of additional owner, Home address number and street, City, State, State, State, Title, and Title field will be applied to record the rights or responsibilities of each party.
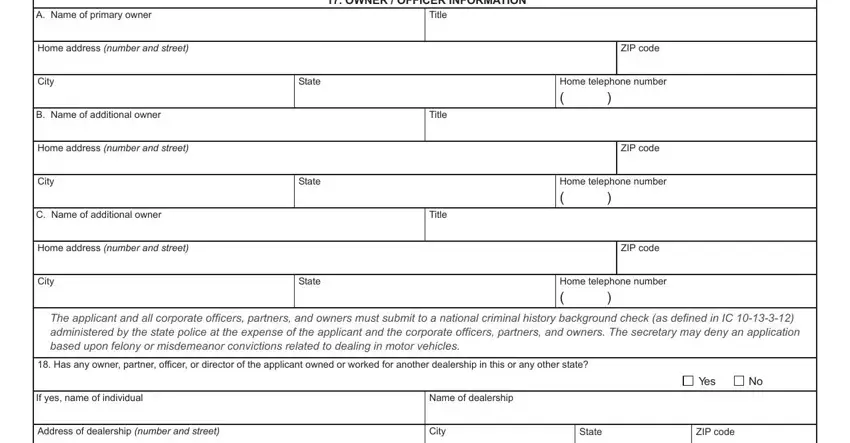
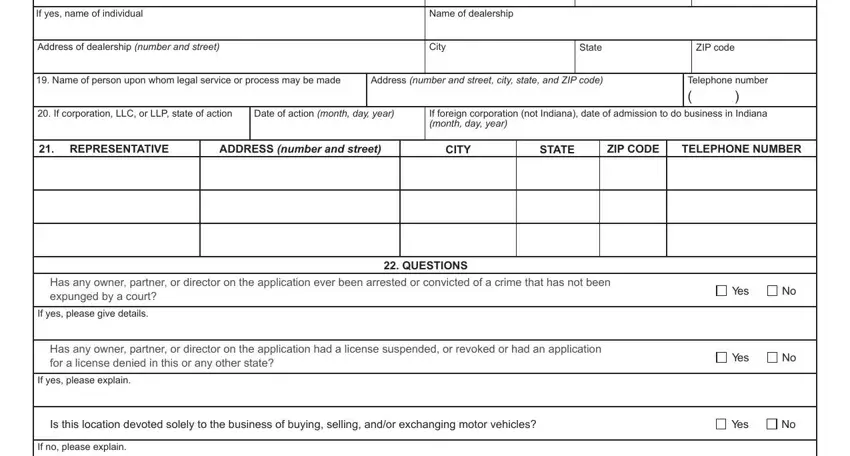
Fill out the template by reviewing all these fields: If yes name of individual, Name of dealership, Address of dealership number and, City, State, ZIP code, Name of person upon whom legal, Address number and street city, Telephone number, If corporation LLC or LLP state, Date of action month day year, If foreign corporation not Indiana, REPRESENTATIVE, ADDRESS number and street, and CITY.
Step 3: Press the "Done" button. Now you may export your PDF form to your electronic device. Additionally, it is possible to send it through electronic mail.
Step 4: Come up with a minimum of a few copies of the file to prevent any possible troubles.
